

If you are at all squeamish or cannot handle EXTREMELY graphic content, click the back button now. The images contained in this post are not for the faint of heart.
And click here to view posts related to the vax and the vaccine.
As a 30 year old woman, I have had my fair share of nightmare periods. As someone who grew up with 2 sisters, lived with 4 girls in college and spent plenty of time in the sorority house bathroom, I thought I had just about seen and heard it all.
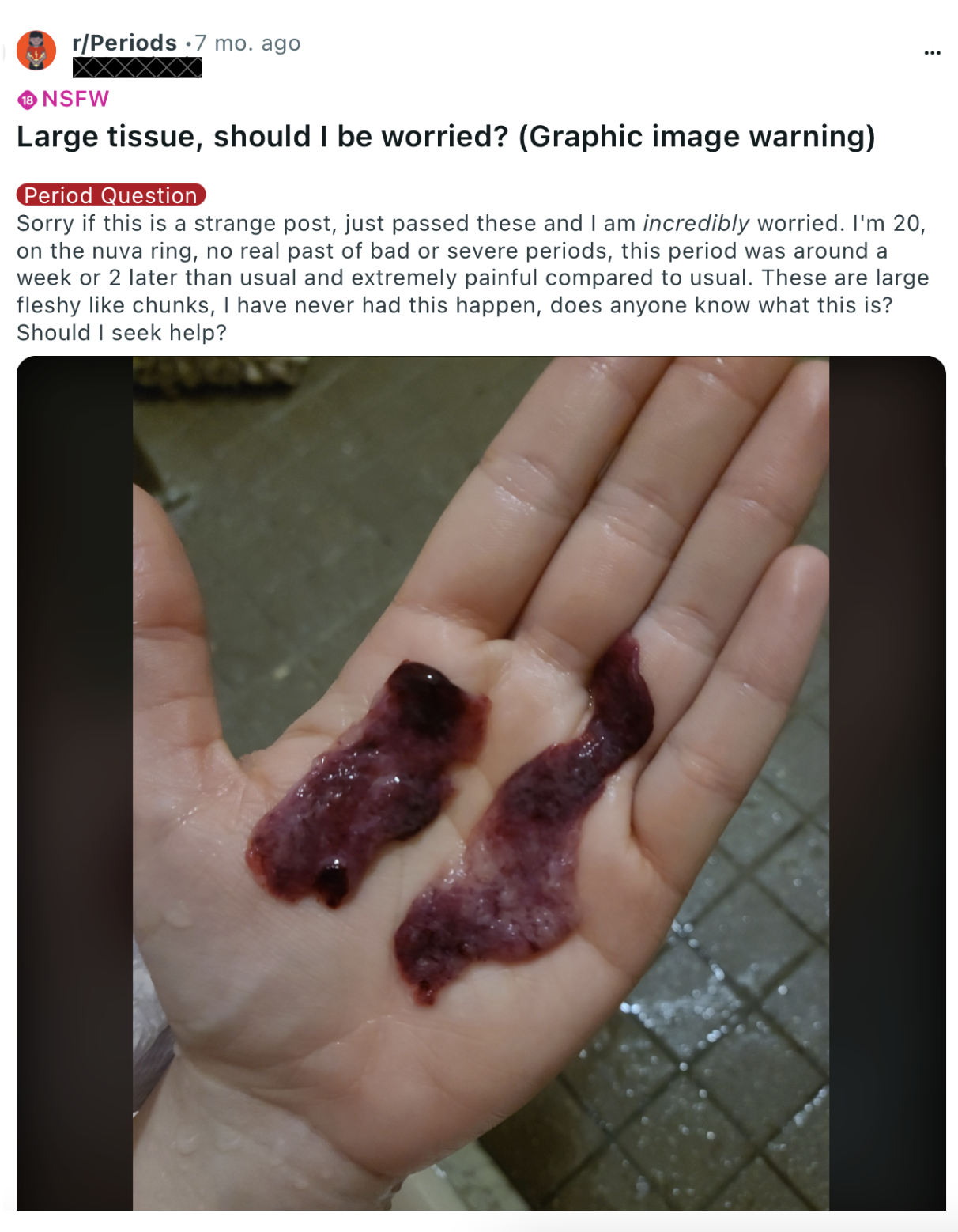
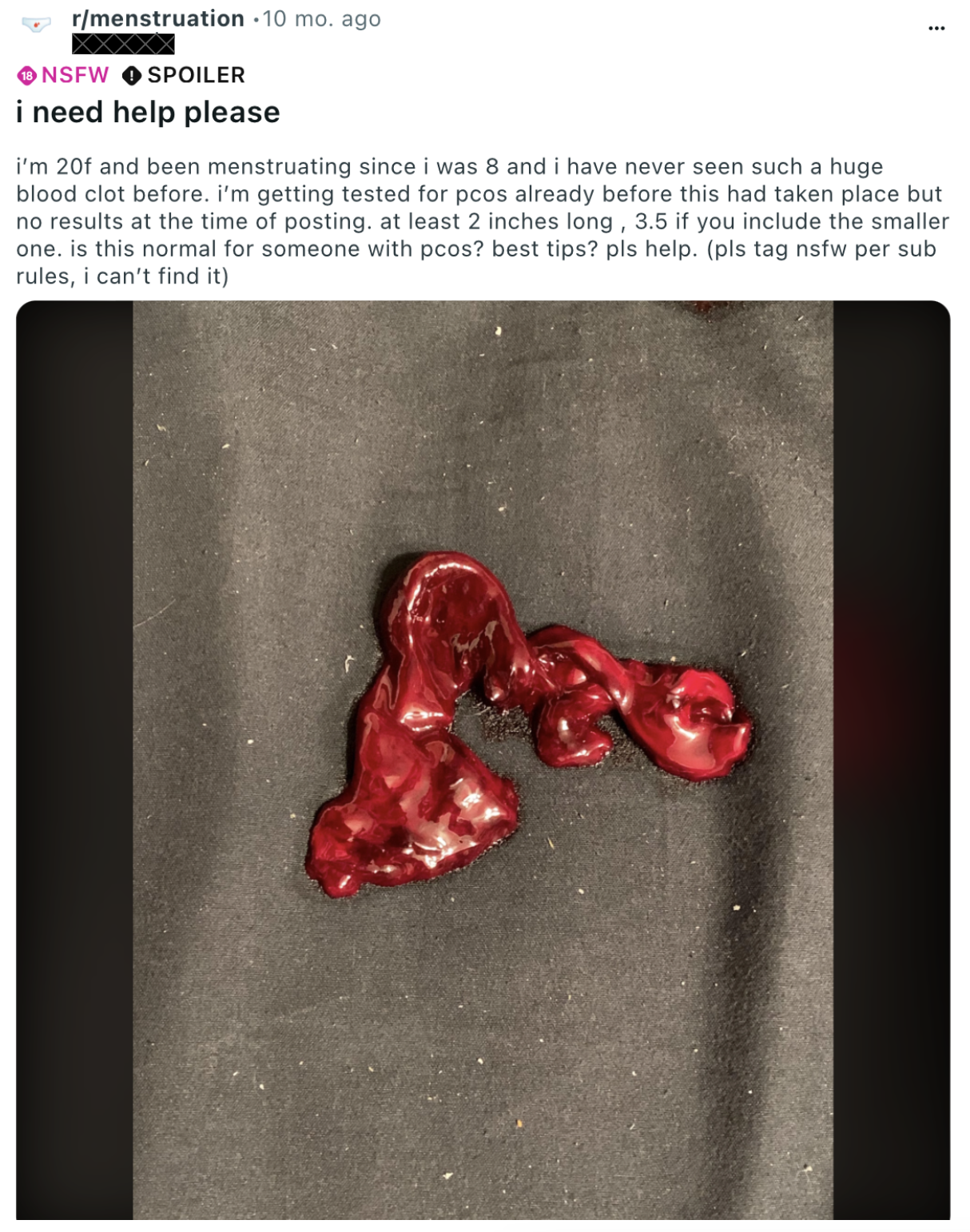
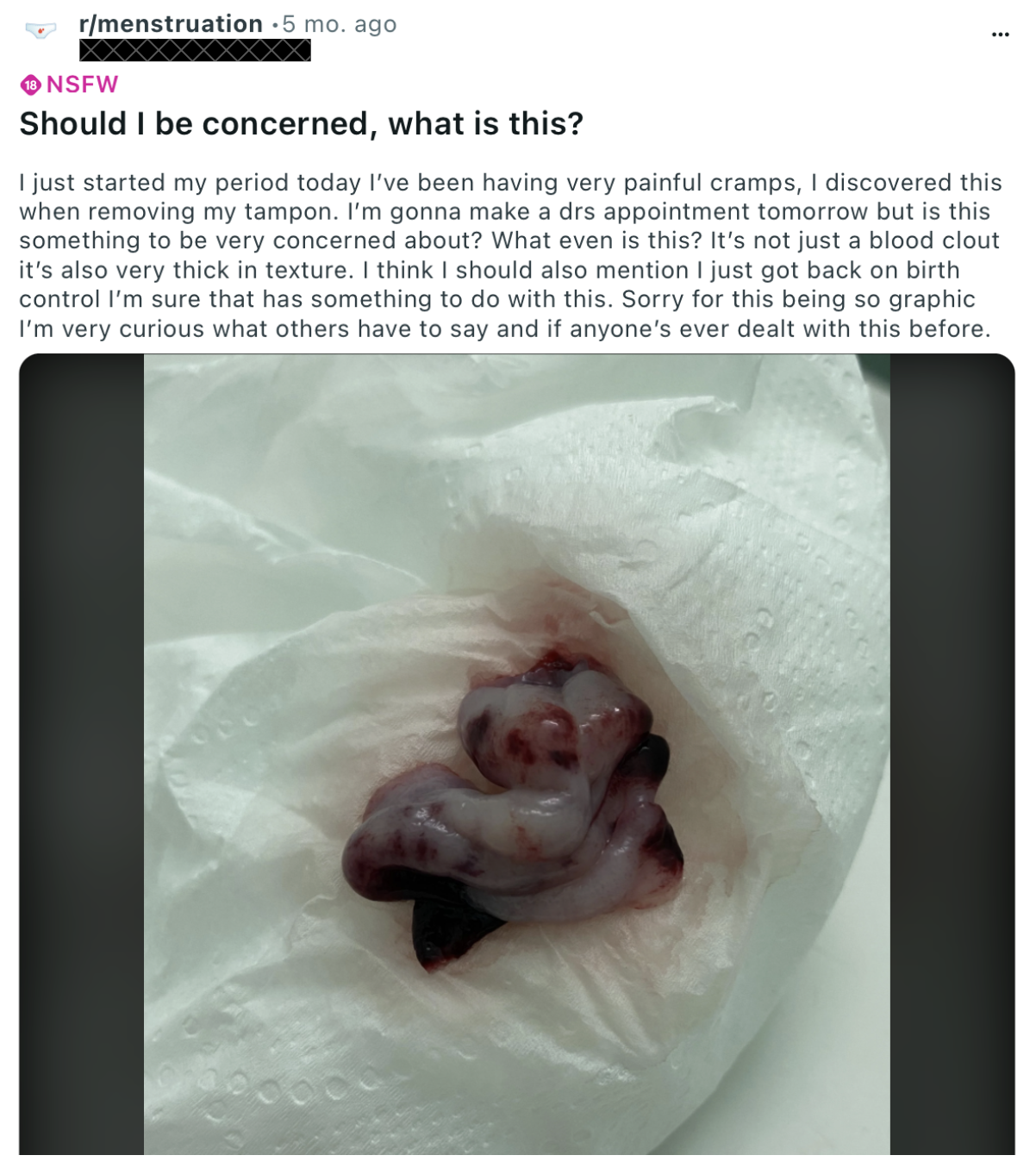
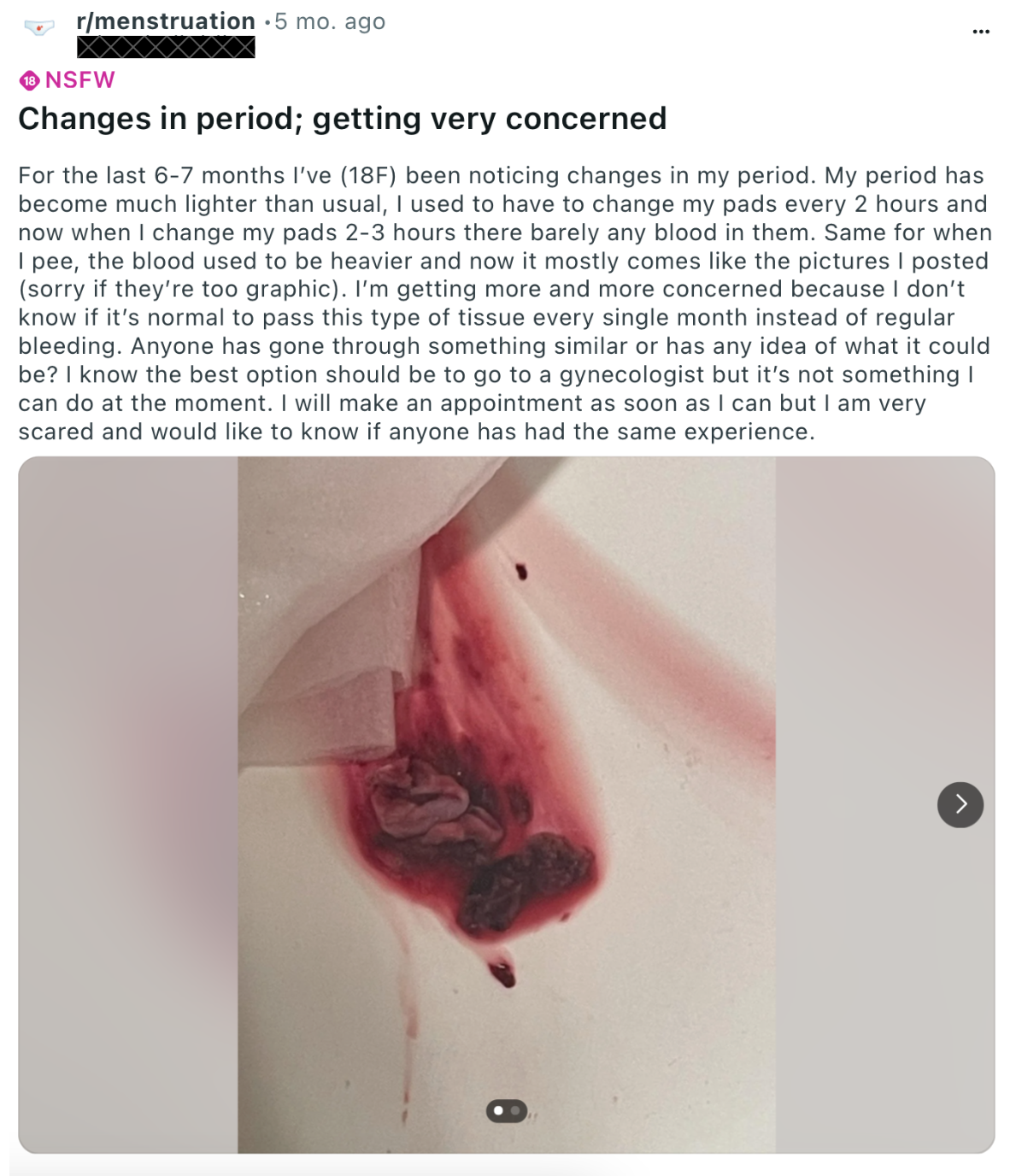
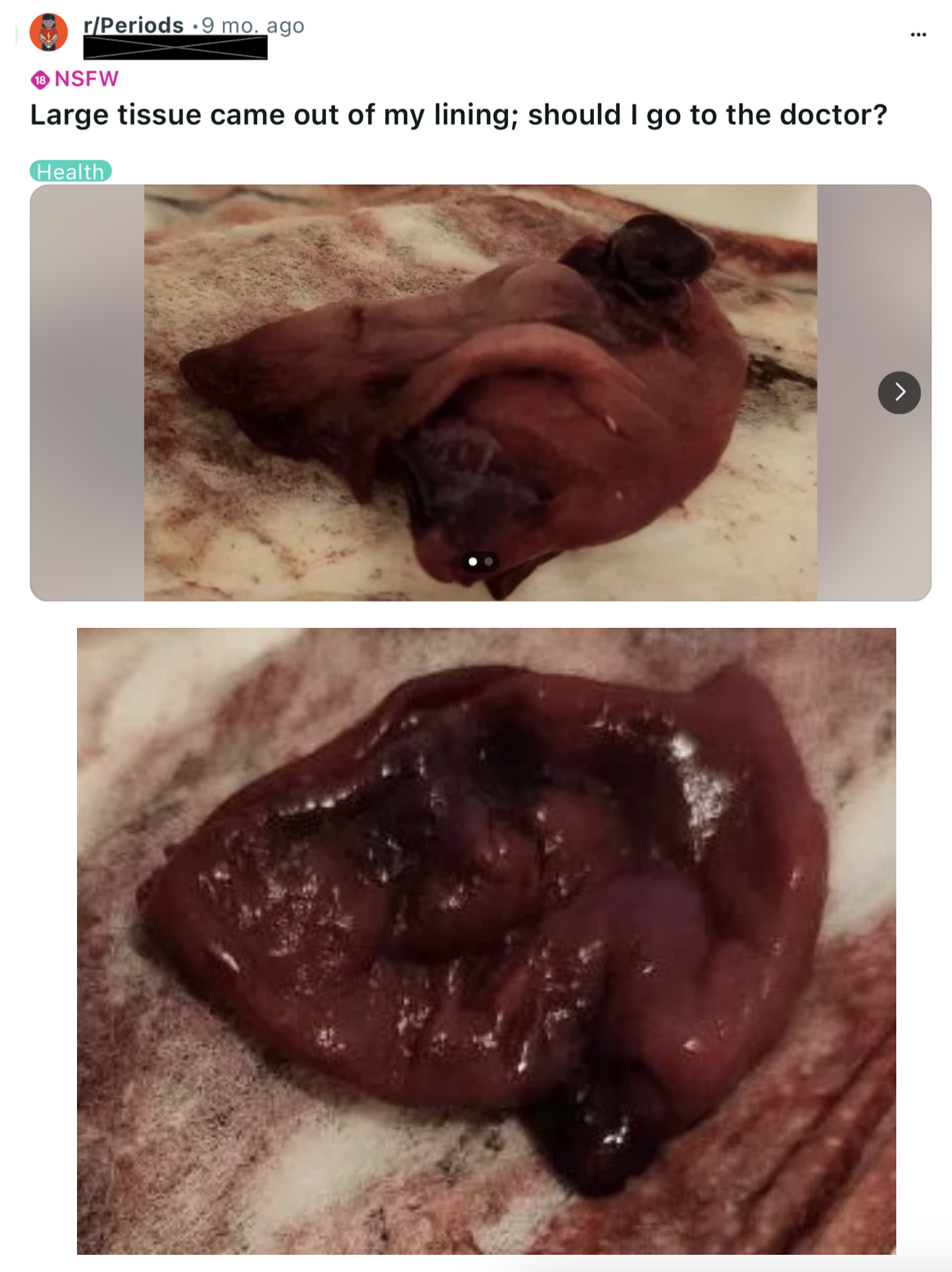
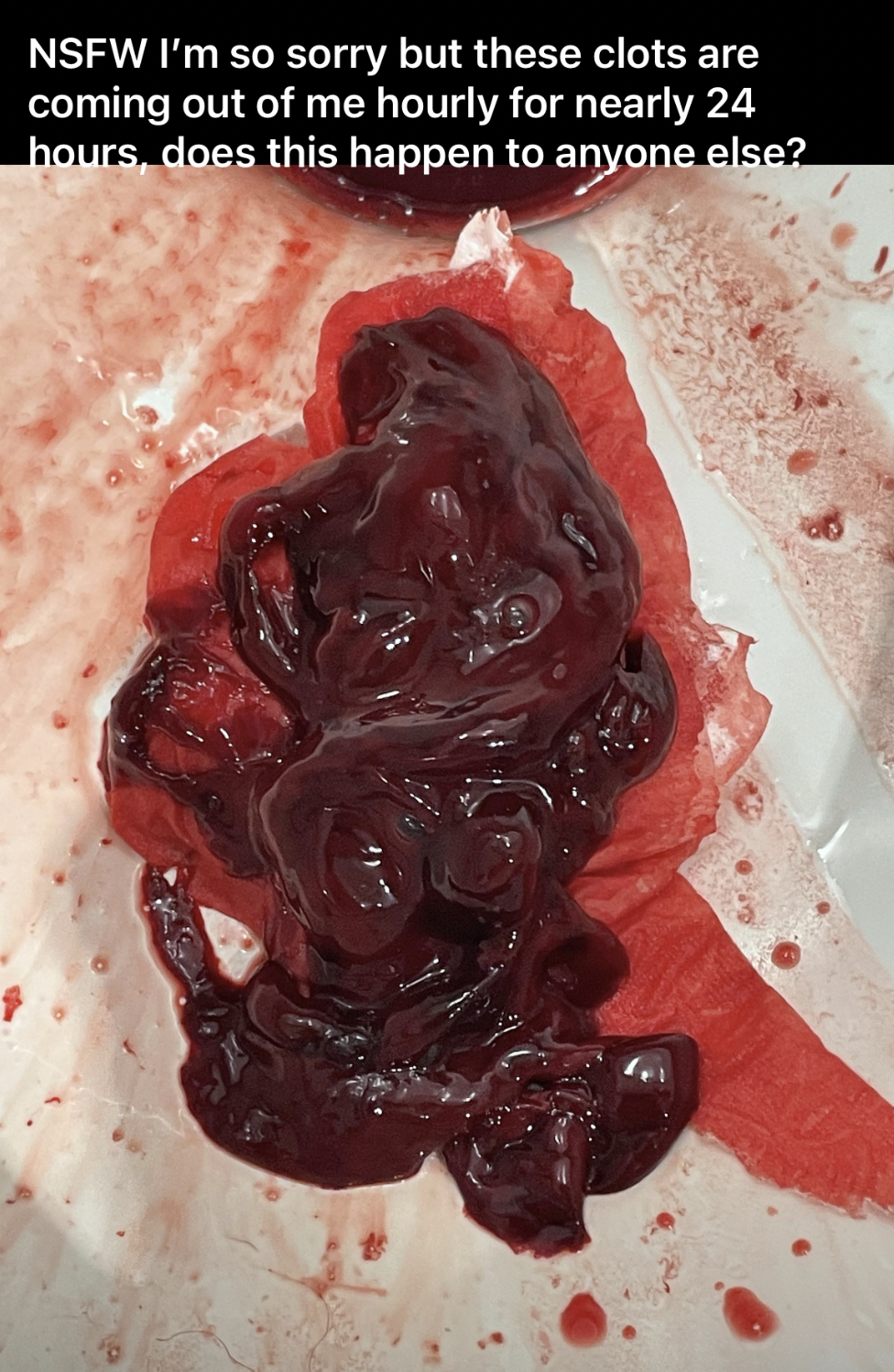
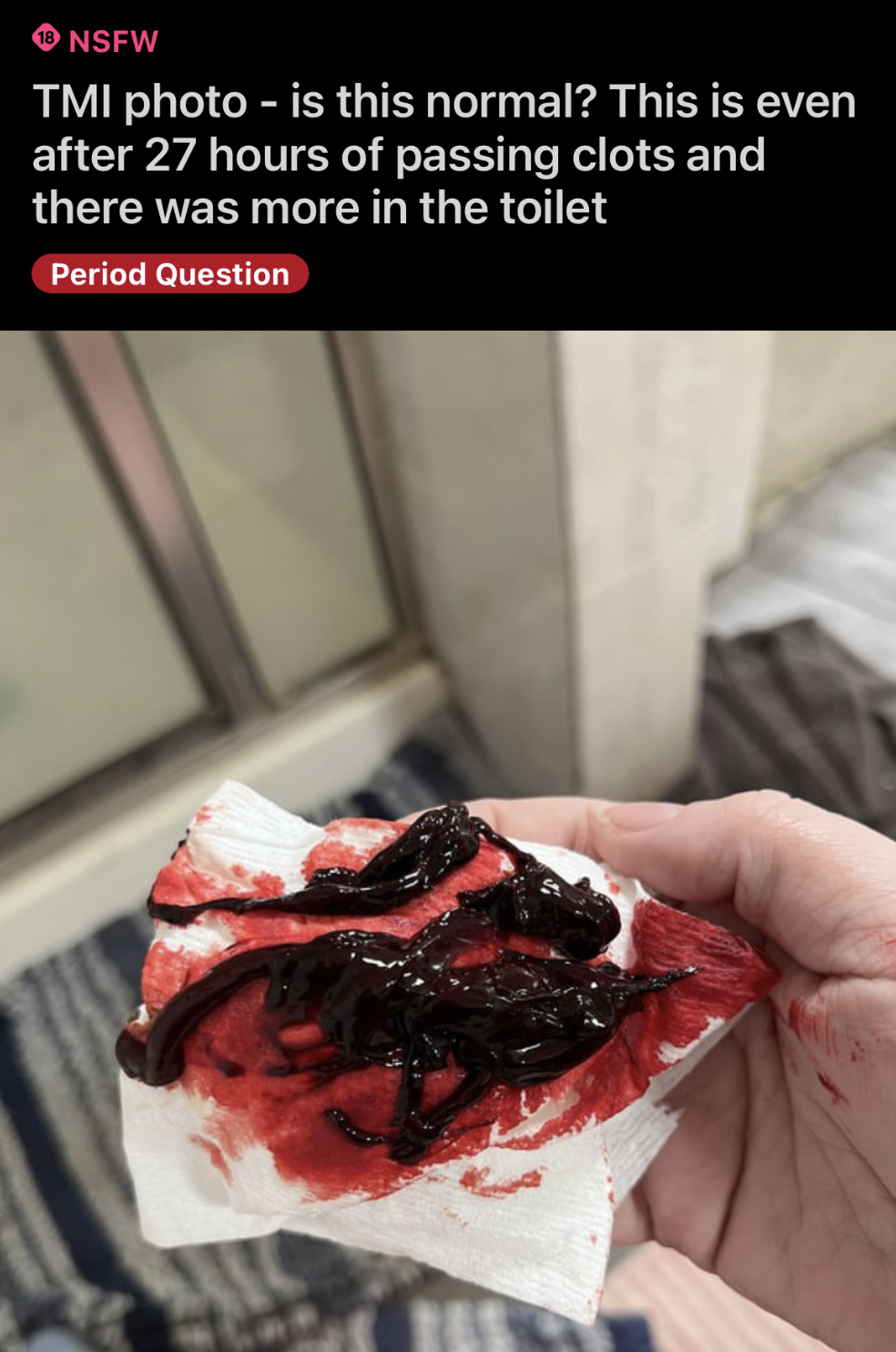
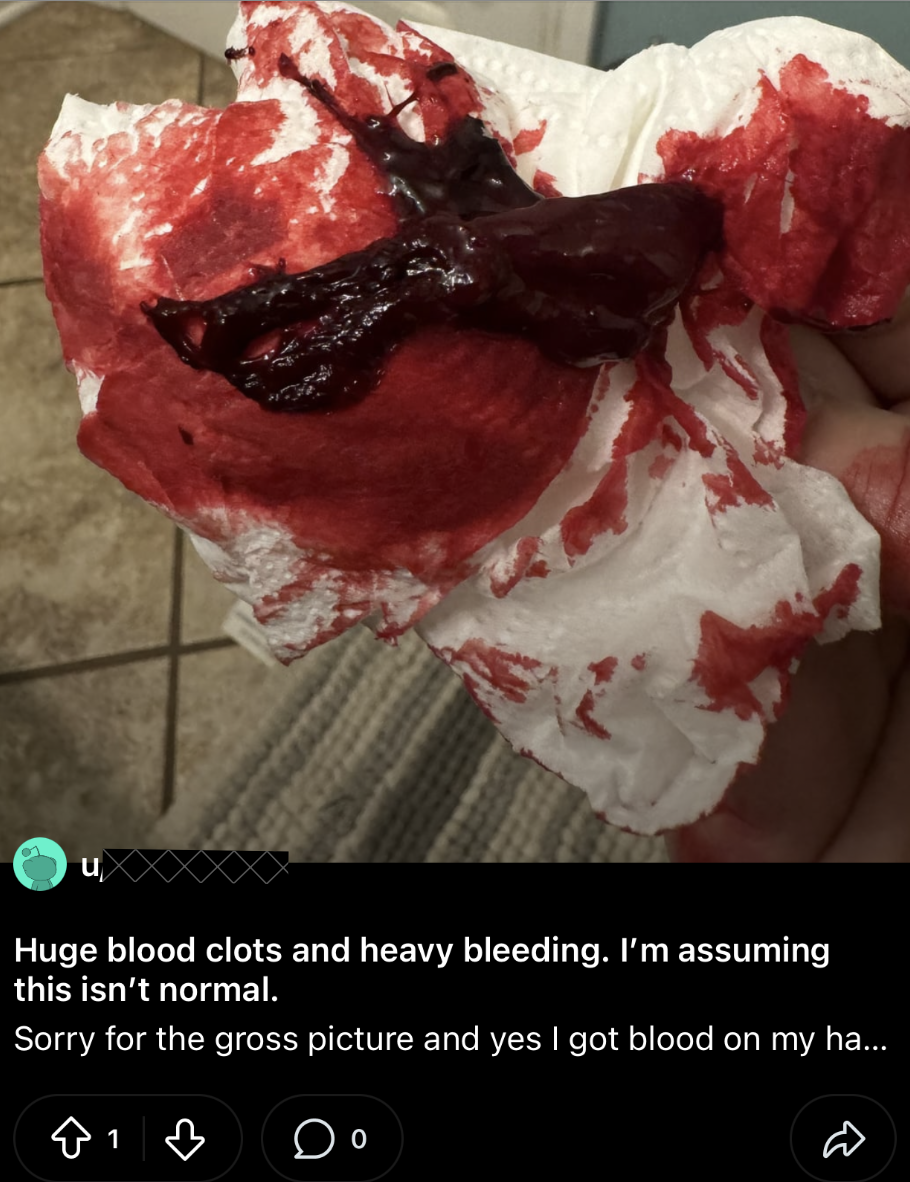
But over the past two years, the posts describing and sharing photos of massive clots and huge pieces of fleshy tissue have been beyond anything I've ever seen or heard.
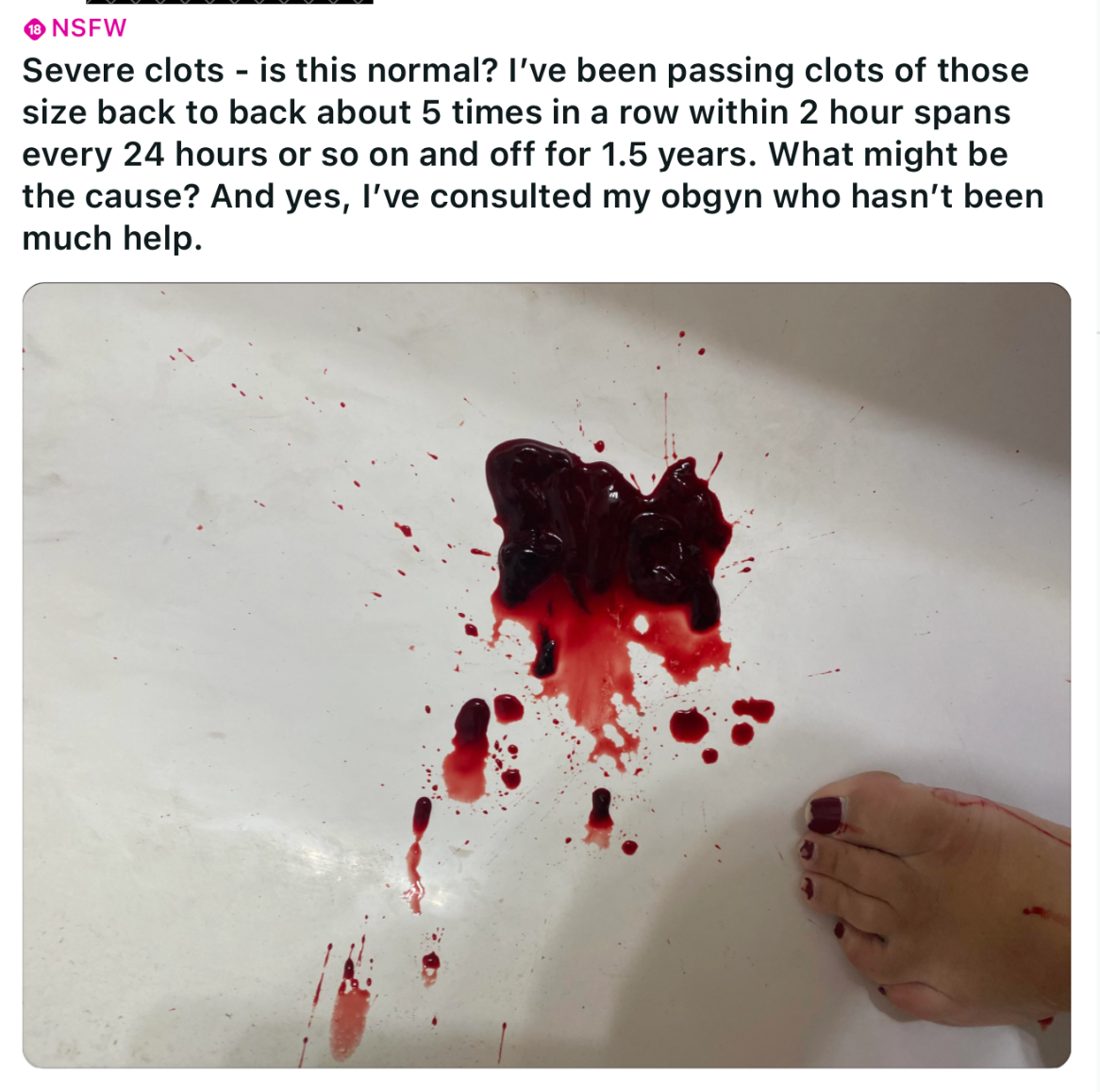
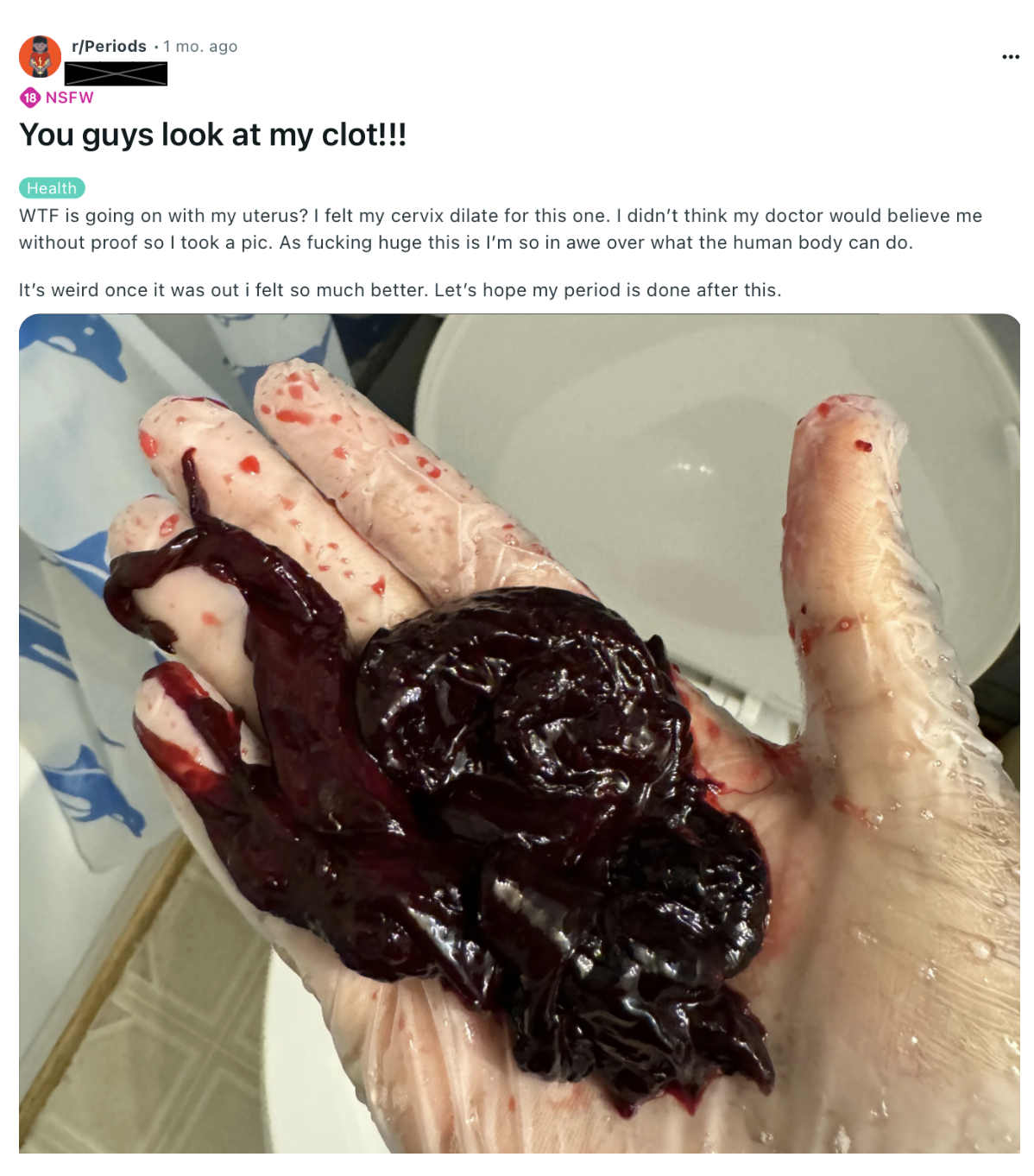
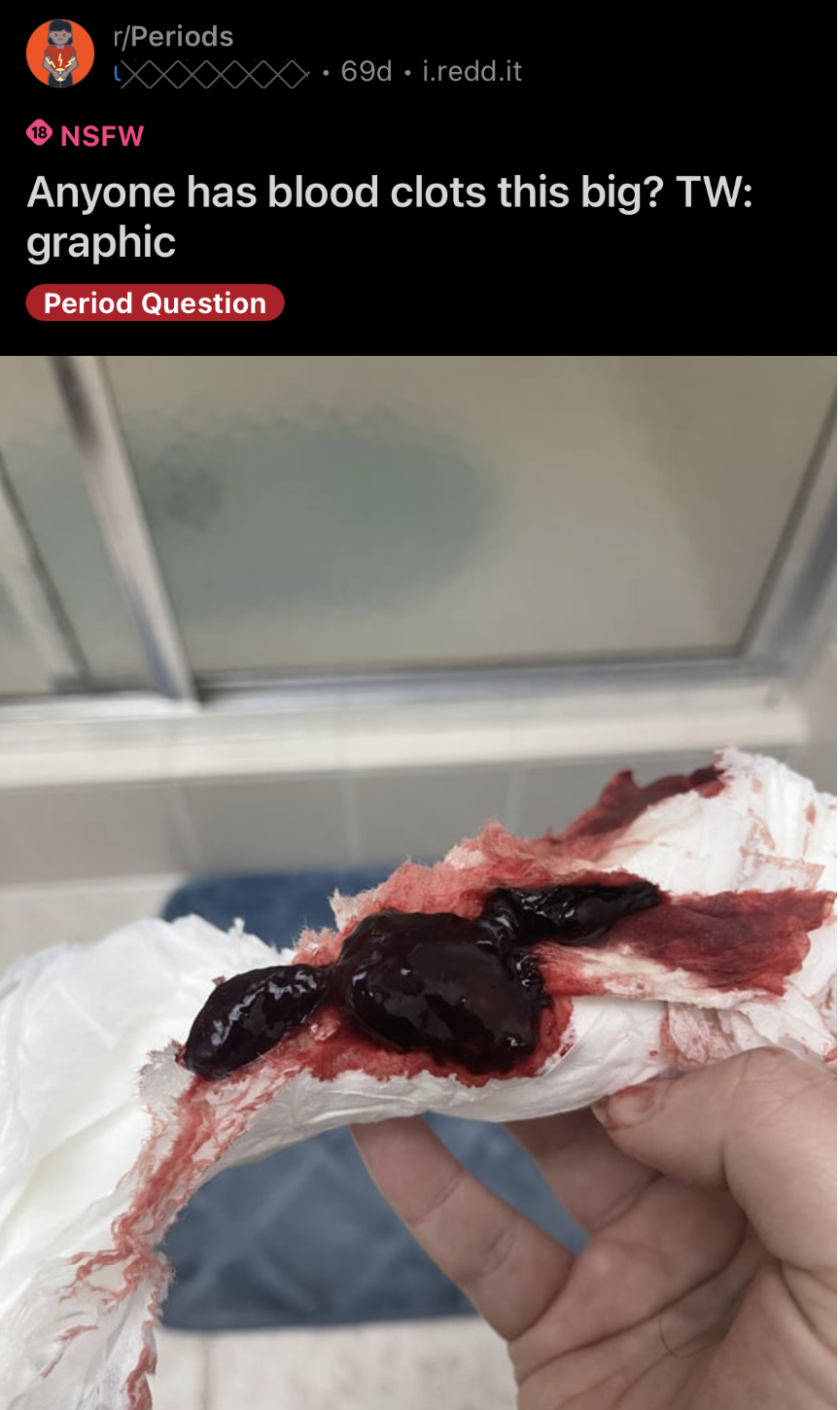
Since 2021, there has been an increasing incidence of posts on r/Periods and r/Menstruation depicting period clots the size of tennis balls and soft tissue clumps the size of golf balls.


These posts are now a daily occurrence, multiple times a day. And, as a woman whose had hundreds of periods, they are terrifying.




Medical literature and professionals tell us that period clots happen, but as long as they are not chronic and don't exceed the size of a quarter, they are nothing to be concerned about.

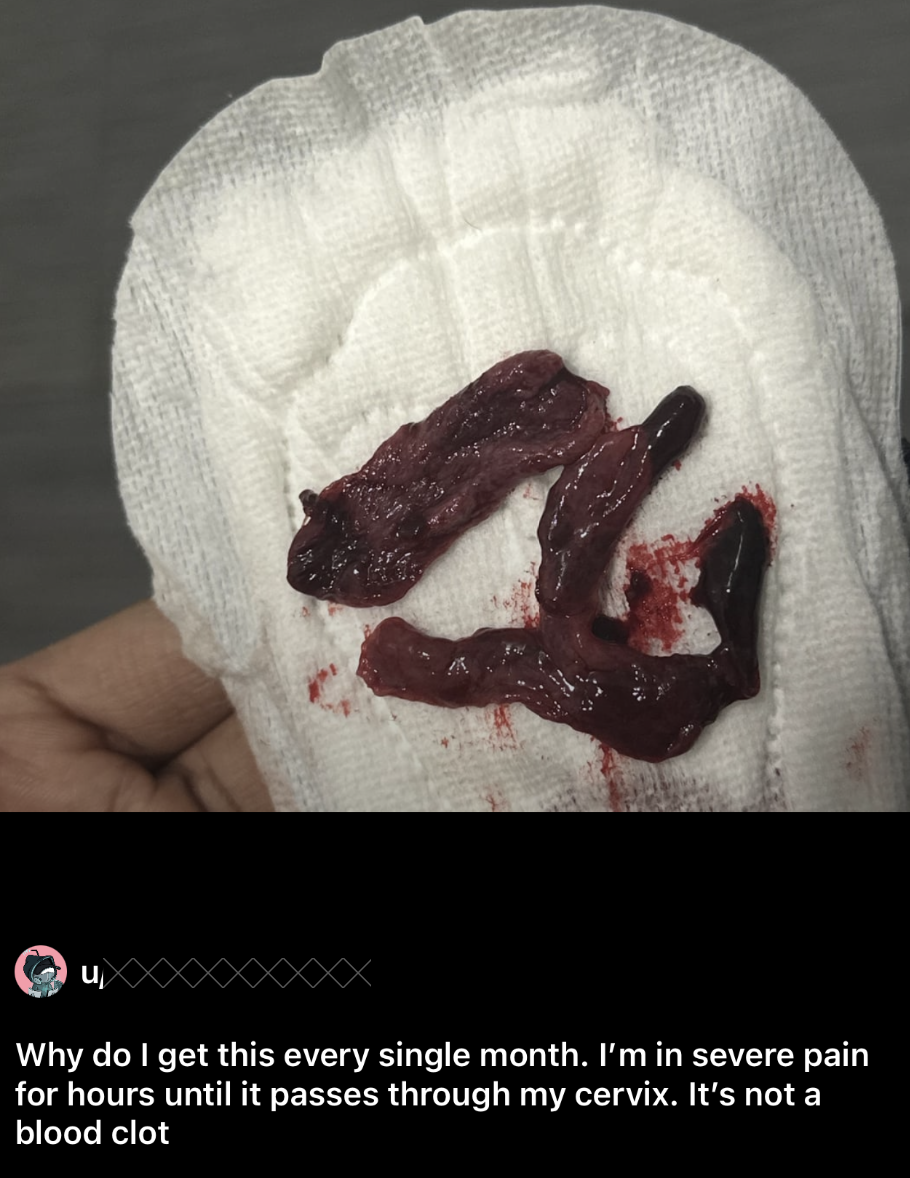
But as you'll see from the posts, what we are seeing is an entirely different animal. These are massive clots and massive pieces of uterine tissue that are not only concerning, but extremely painful.
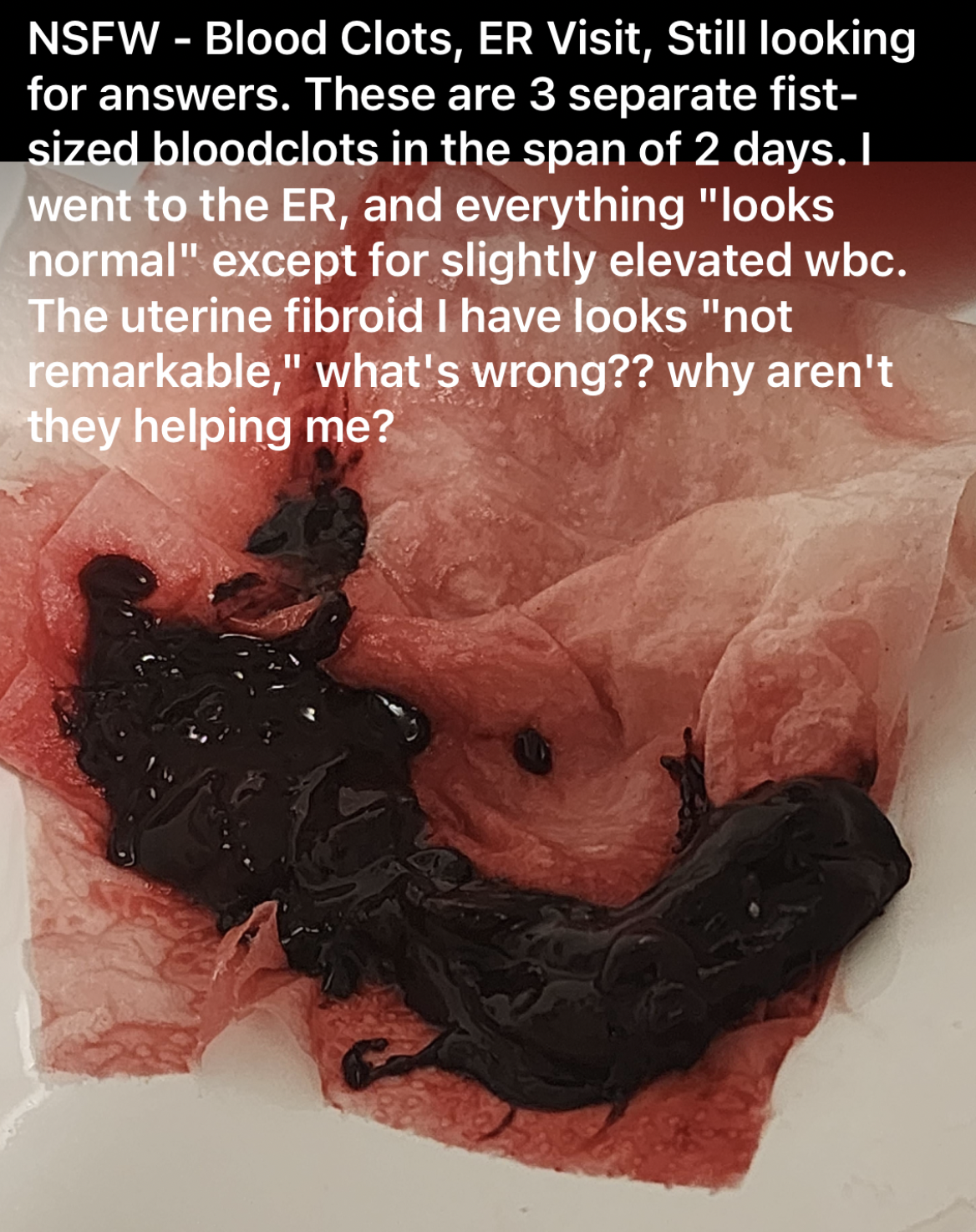
There are hundreds of posts from women each week who are terrified and seeking help from medical professionals only to walk away with no answers and no way to stop it or heal themselves. No one seems interested in even educating them about what is occurring and why.

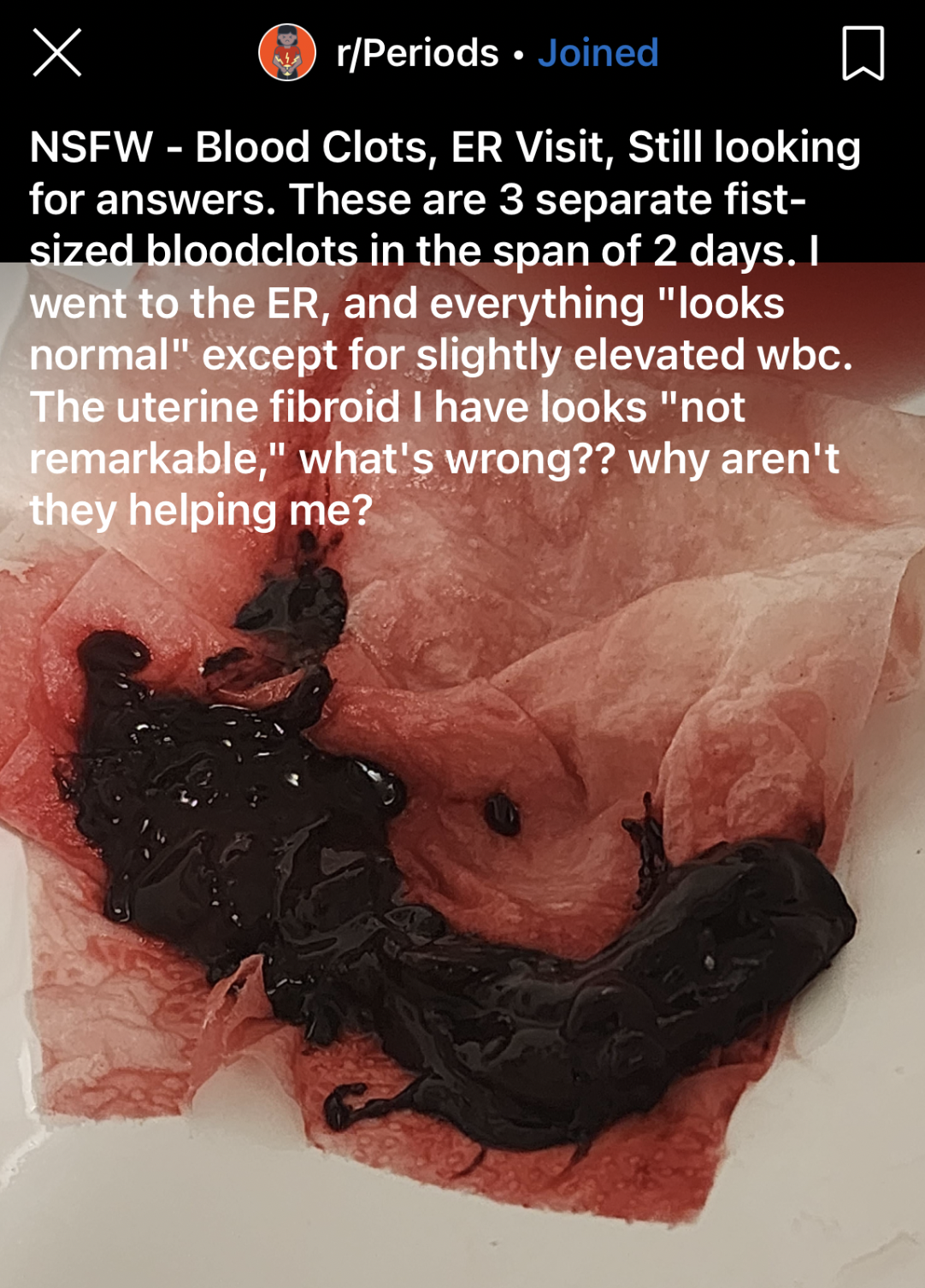
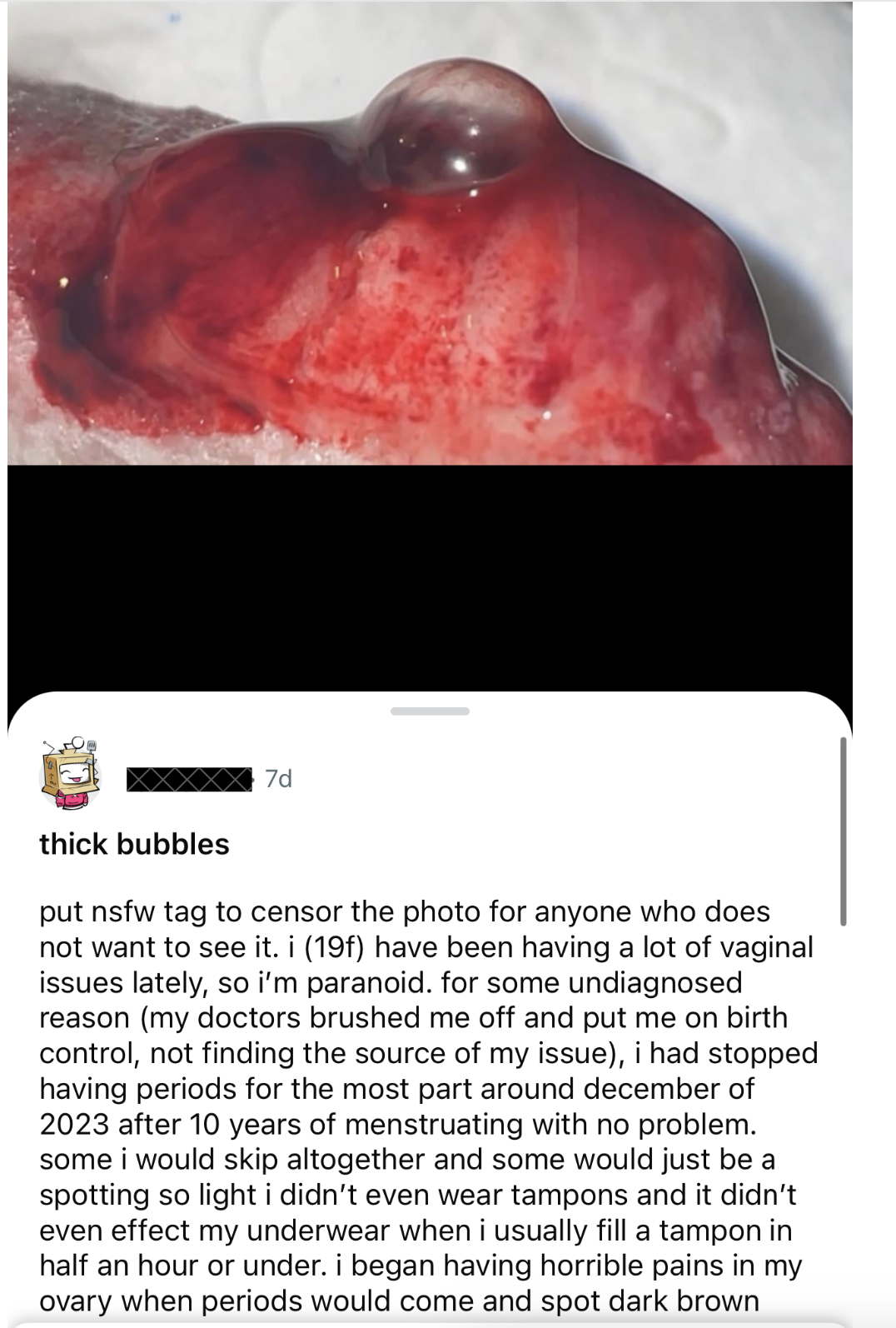


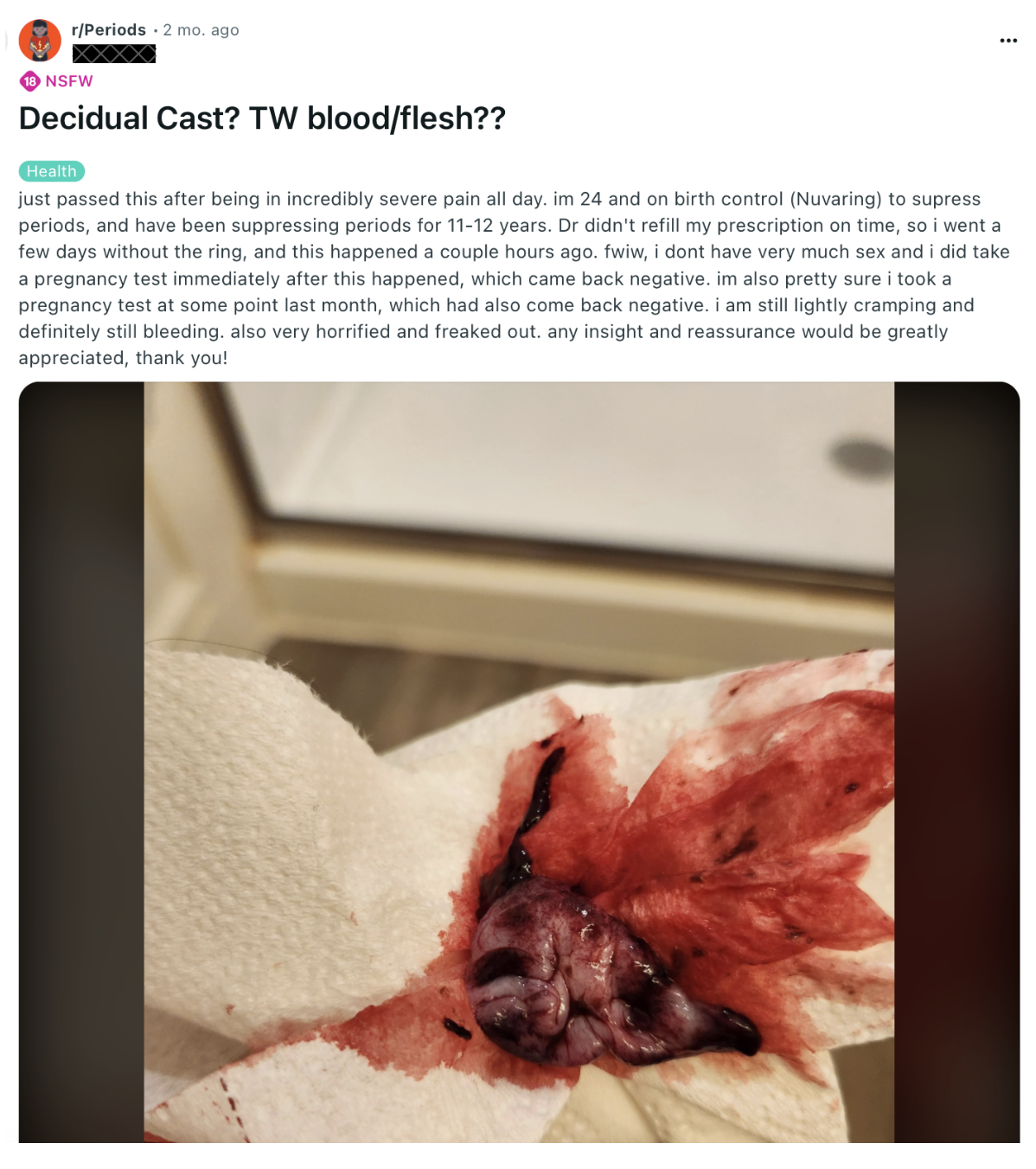
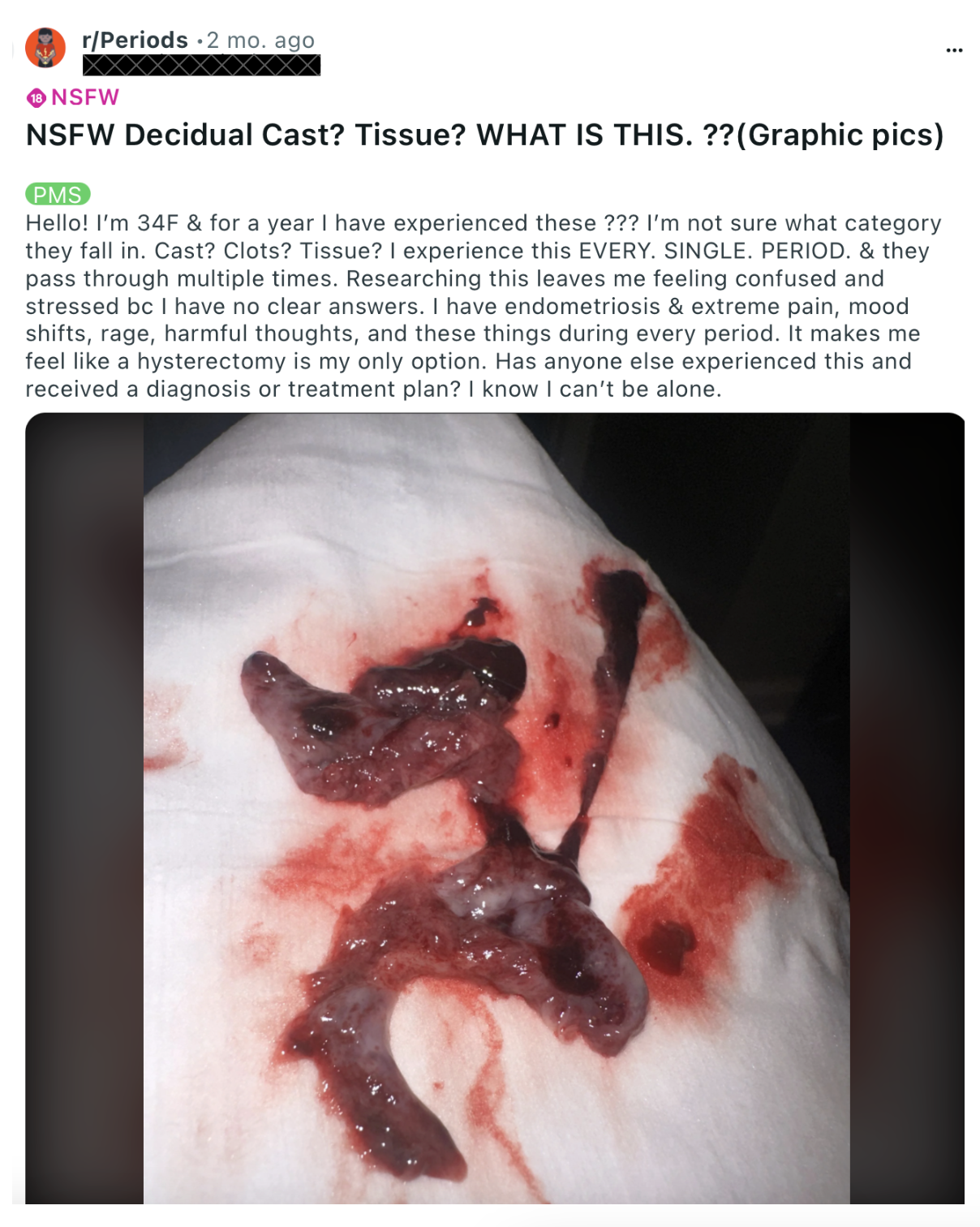
Doctors continuously brush the tissue masses off as "decidual cast", explaining they are totally normal, harmless and are not a sign or indication of any problem. The massive blood clots are also dismissed as normal. When patients continue to experience these with extreme pain and increasing frequency, doctors might blame PCOS or endometriosis (abnormal thickening of the lining of the uterus), tell them to take their birth control and send them on their way.
But not one will say what is causing it to suddenly occur, what it indicates about the health of the uterus, or what it indicates about the health of the body as a whole. And the only treatment options are birth control, surgery or removal of the ovaries all together (a surgery which is becoming horrifyingly common for young women - but that's a post for another day).
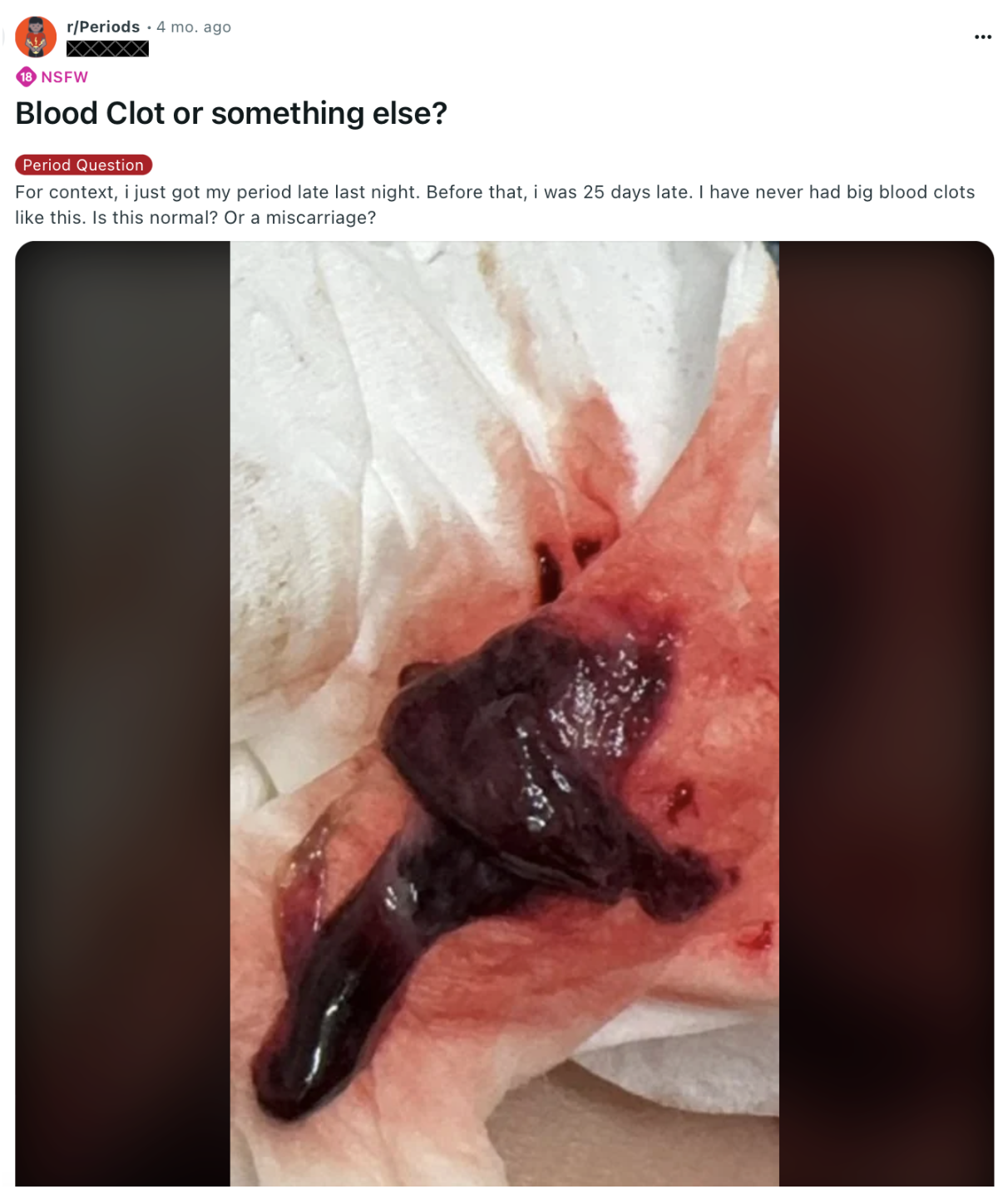

These are not genetic conditions, these are occurring in women who have had normal periods their whole life, and are suddenly, seemingly out of the blue, experiencing these extreme and distressing changes in their menstruation.

Not one woman has been given an answer or explanation as to what is happening inside their body to cause such sudden, abnormal, painful periods. How can doctors be so mystified by menstruation? How can the only explanation be, "it just happens sometimes - it's nothing to worry about", when it reality, it's never happened to any of these women before, and they are extremely worried.


And thousands of the posts mention the clots began after receiving vaccination.
What is really happening here?
So, there are a few questions we need to answer.
- What actually happens throughout a healthy, normal menstrual cycle at the cellular level, and what could interfere with this process?
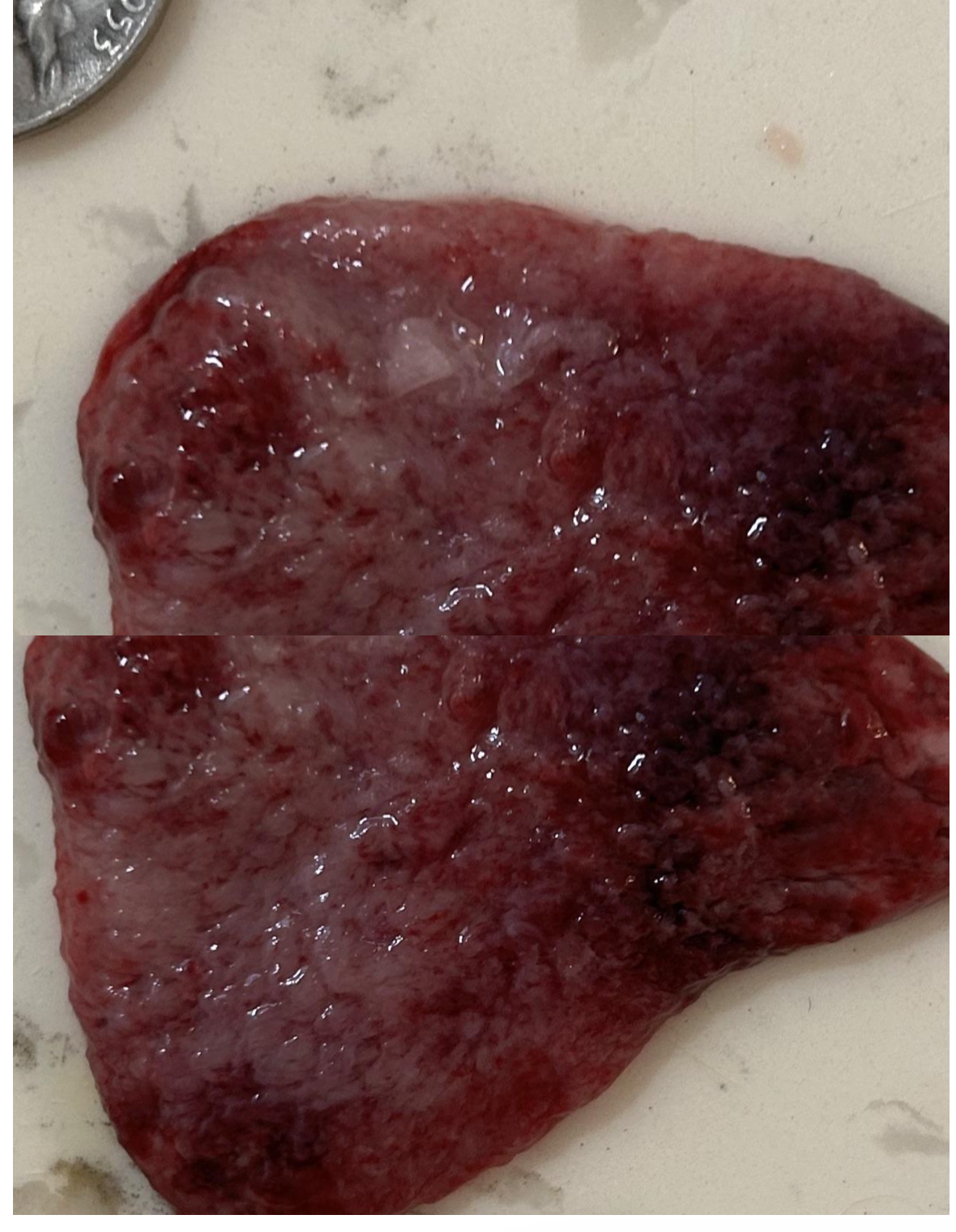
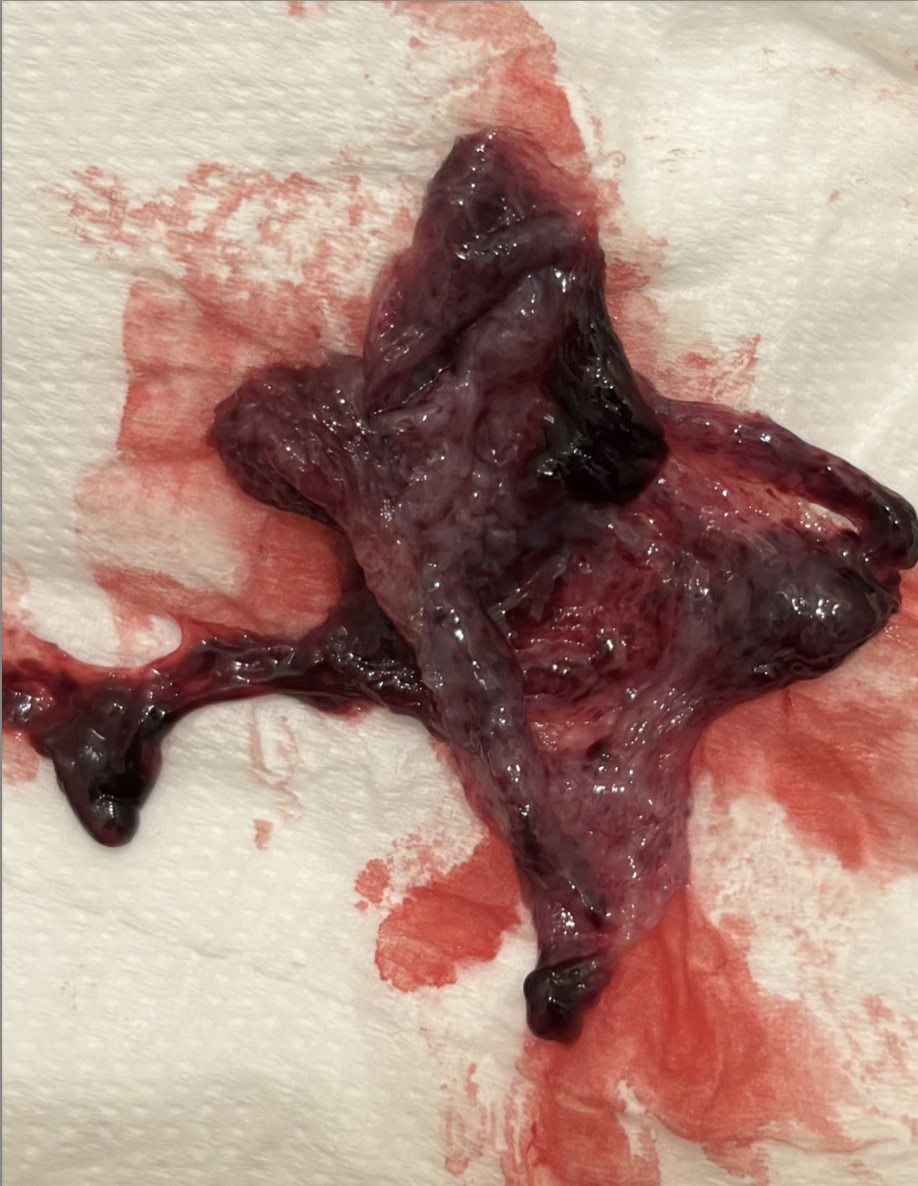
- What is the difference between the uteruses of the women passing massive, coagulated clots of blood larger than golf balls, and the women passing large pink, fleshy tissue casts?
- At the cellular level, what is driving the production of the blood clots?
- What is causing cells to replicate so quickly in the uterus and then be entirely sloughed off to produce the tissue pieces?
- What do these signs and symptoms indicate about the health of the uterus?
- What do they indicate about the health of the body?
- How could vaccines play a role in either the formation of clots or the passing of abnormally thickened tissue?
What Occurs During A Healthy, Normal Menstrual Cycle At The Cellular Level
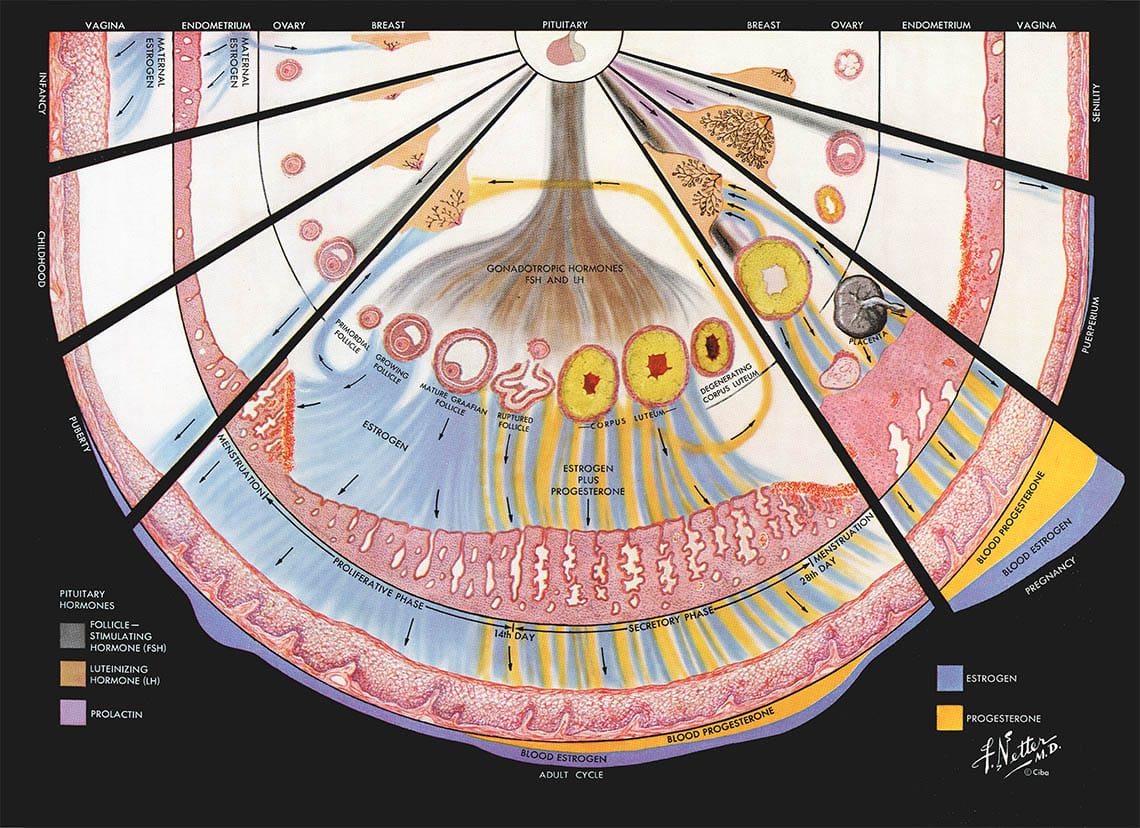
During the menstrual cycle, the inner layer of the endometrium is built up under the influence of estrogen and then “deciduualizes” (differentiates) in response to progesterone in preparation for a possible pregnancy.
This is what allows the body to produce a placenta and the amniotic sac that will hold the fertilized egg and allow it to exist in an entirely protected environment during pregnancy.
If the egg isn't fertilized, a drop in progesterone triggers a controlled breakdown of this lining. The progesterone causes the capillaries in the endometrium to constrict, so that the smallest capillaries become too small for blood flow. The smallest capillaries are the newest, and they only feed the cells which make up the outer lining. When they close off, the cells making up the lining experience hypoxia (lack of oxygen). This paired with the drop in progesterone triggers programmed cell death in the outer layer of cells.
When these cells die, they no longer have the energy to maintain their attachment to the uterus, they become separated from the living system. When this occurs, the blood vessels that were feeding the tiny capillaries become exposed, causing them to bleed. The blood from these capillaries flows out and into the uterus, flushing away the dead cells so that they don't accumulate. This cyclical process allows the body to ensure the environment for a future fetus is as healthy as possible.
So, it's vital that when the endometrial cells of the lining die, the exposed venules are able to bleed and flush them out. The bleeding occurs until new cells have formed, and the cycle is began all over again.
Normally, we're told that fibrin exists in the blood to immediately clot any ruptures or breaks in blood vessels. But endothelial cells produce substances (such as nitric oxide and prostacyclin) that help prevent this clotting from occurring, and instead rely on the regrowth of cells to rebuild the capillary rather than clot it and close it off.
When this system is disrupted, the build up of cells occurs until it is eventually passed. This passing requires the uterus to contract, much like during labor. This can cause extreme discomfort and pain from muscle contractions, nausea, dizziness, extreme weakness, and fainting.
Imaging the Endometrium: Disease and Normal Variants
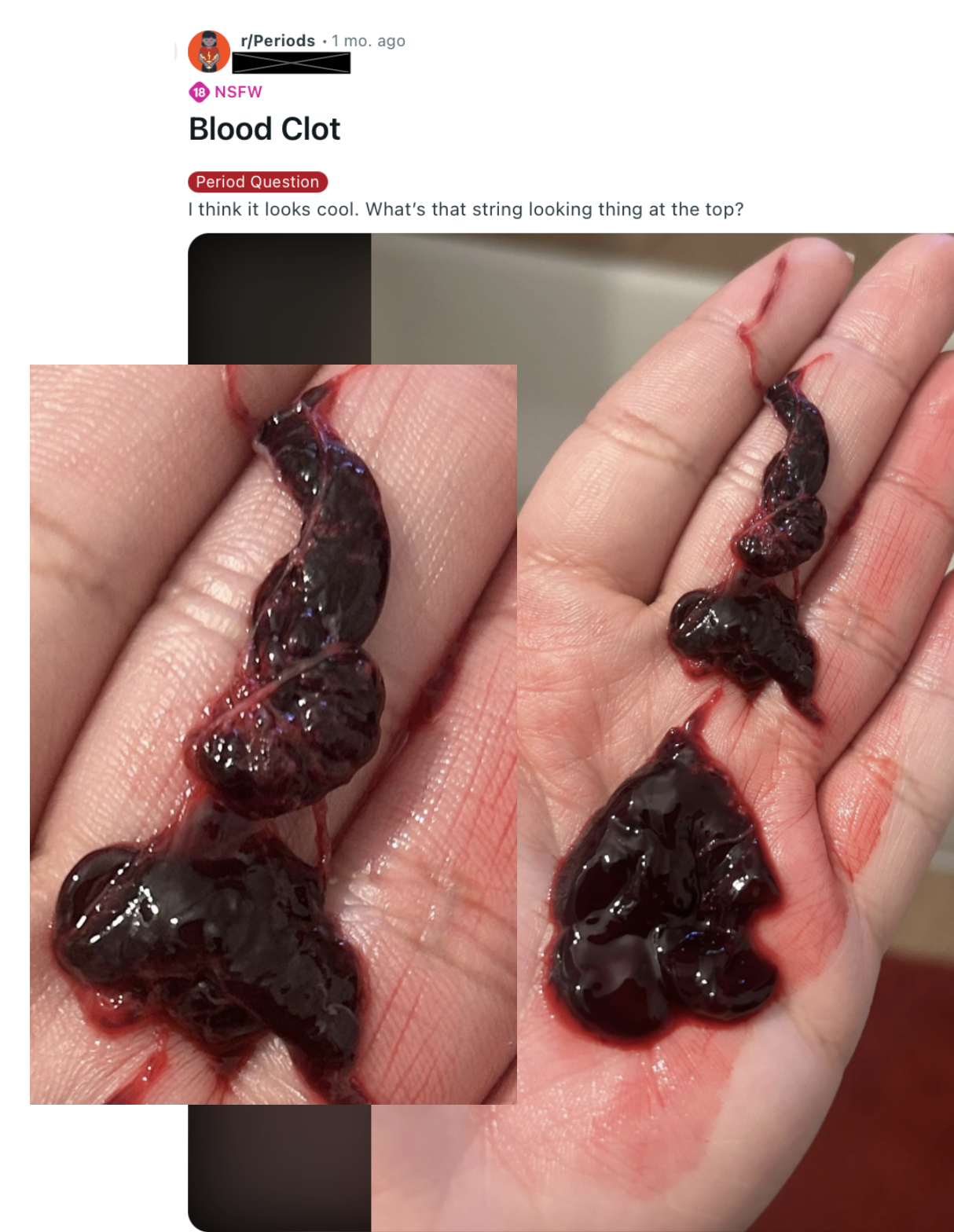
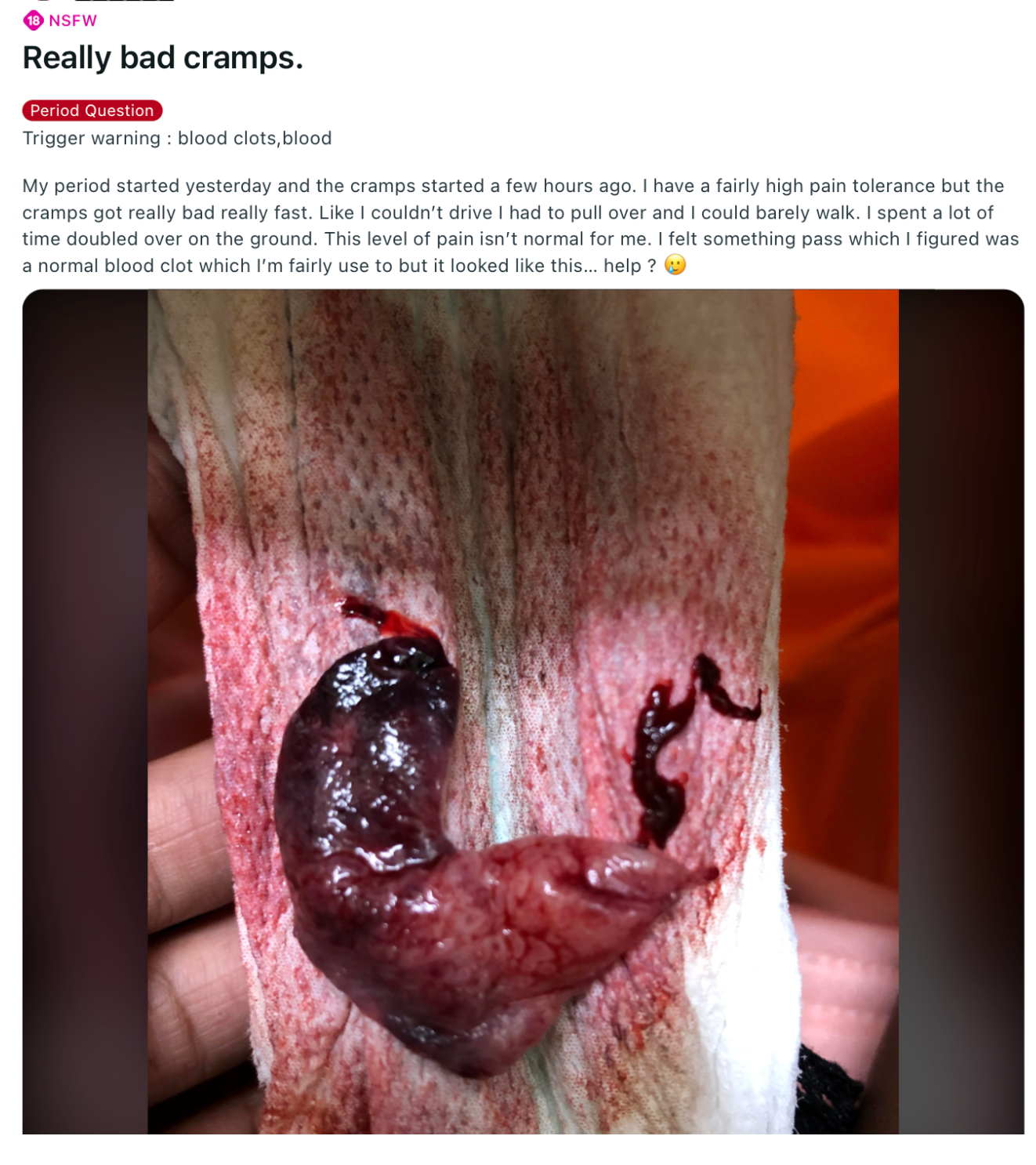
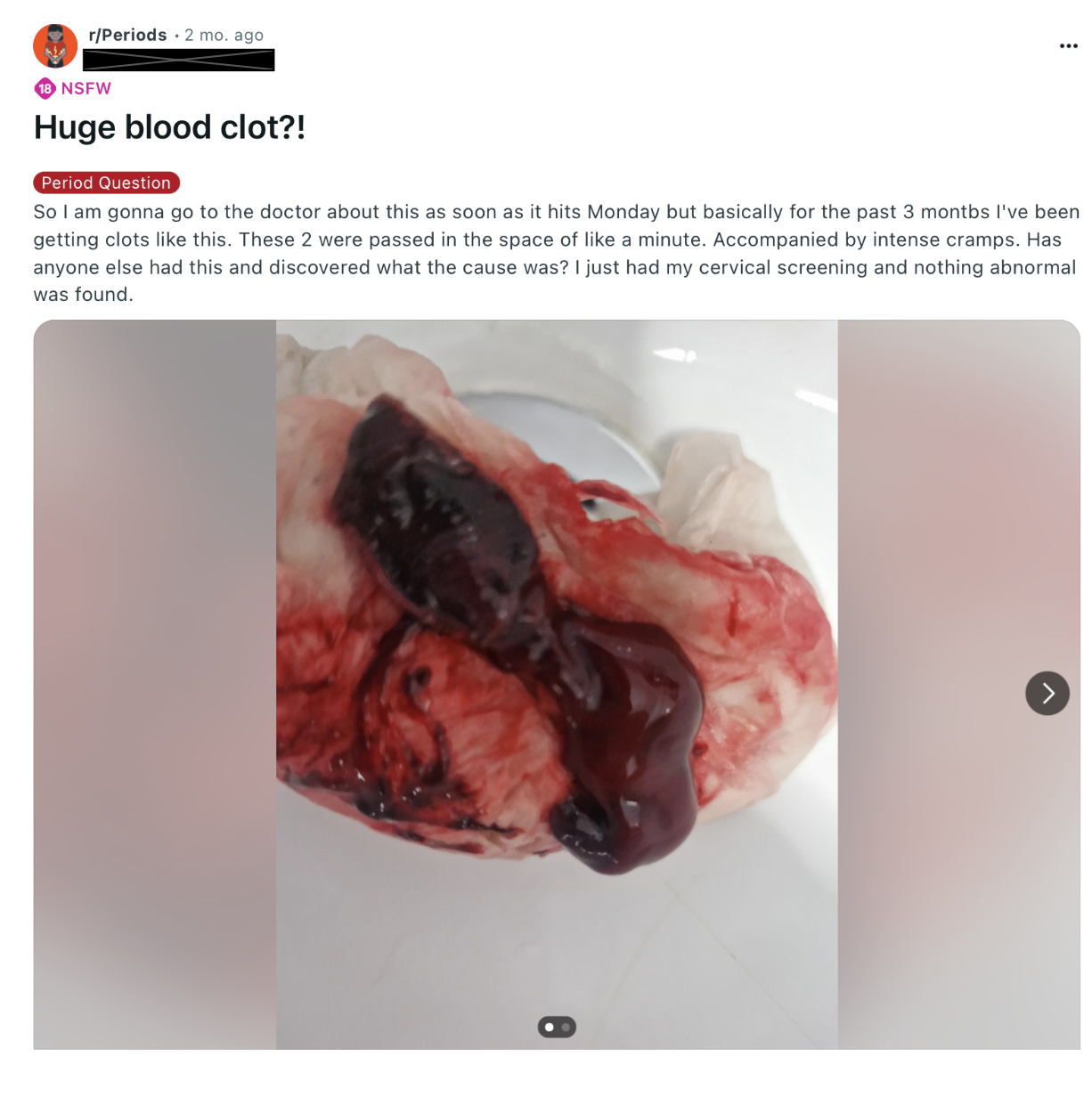
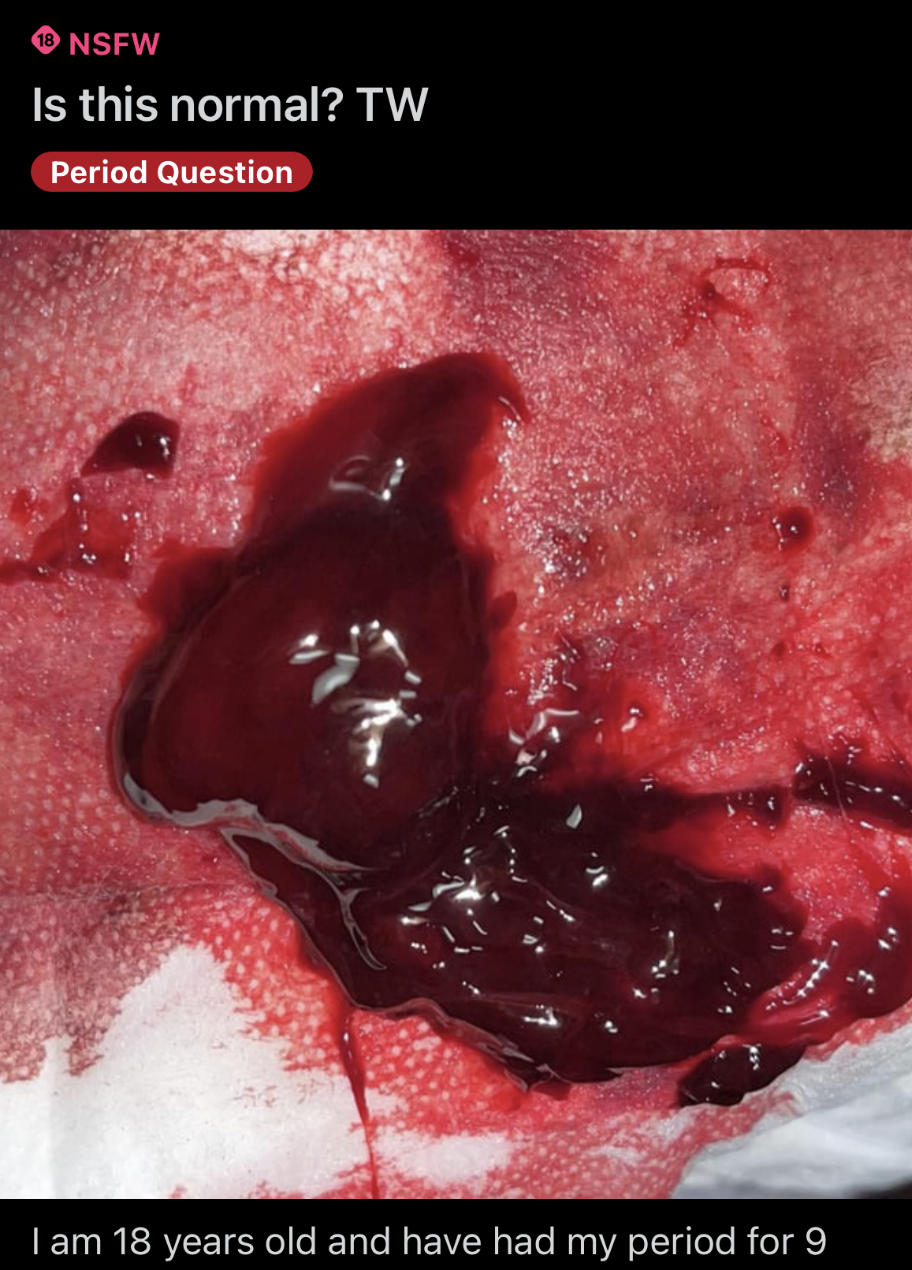
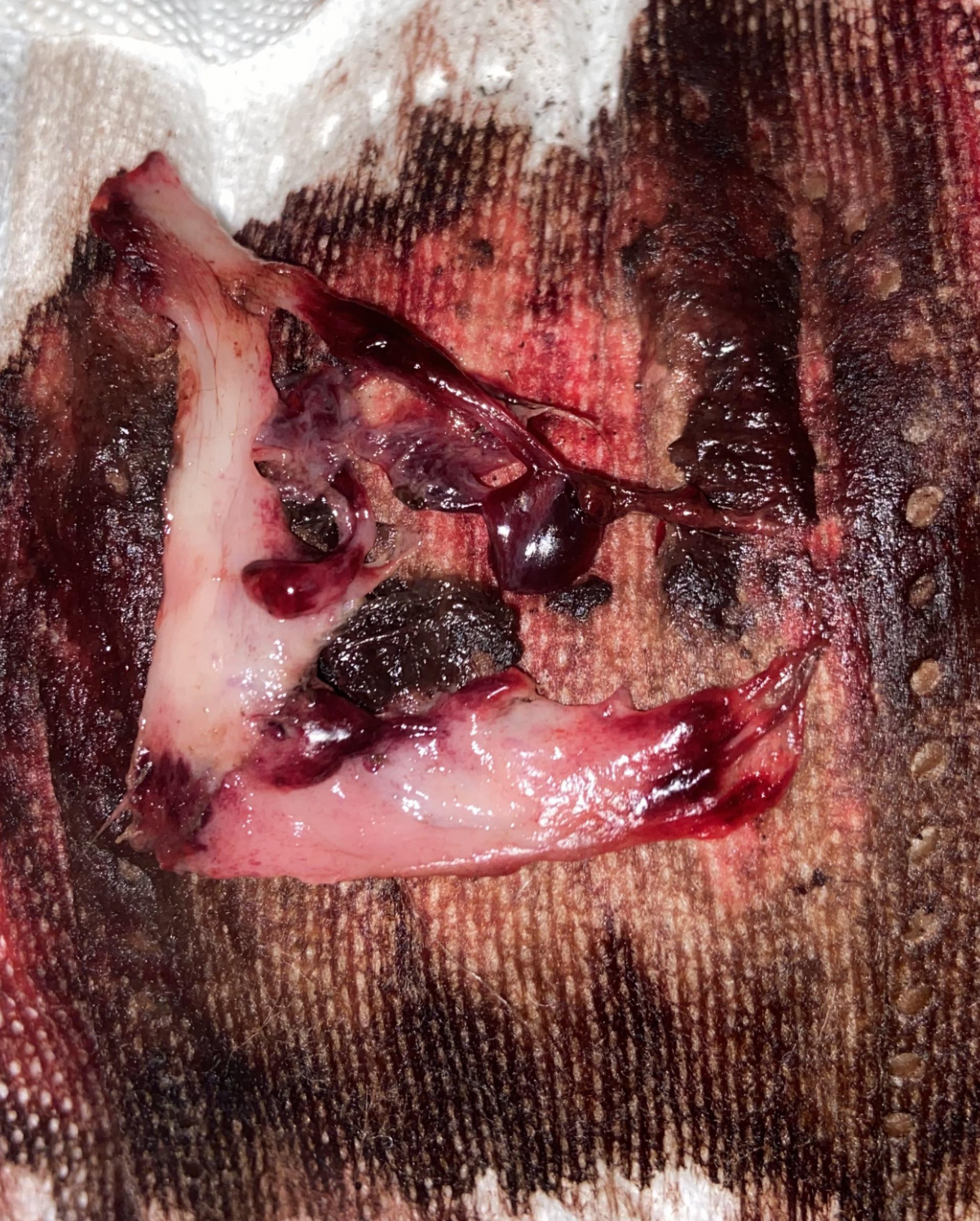
What's the difference between the blood clots and tissue masses?
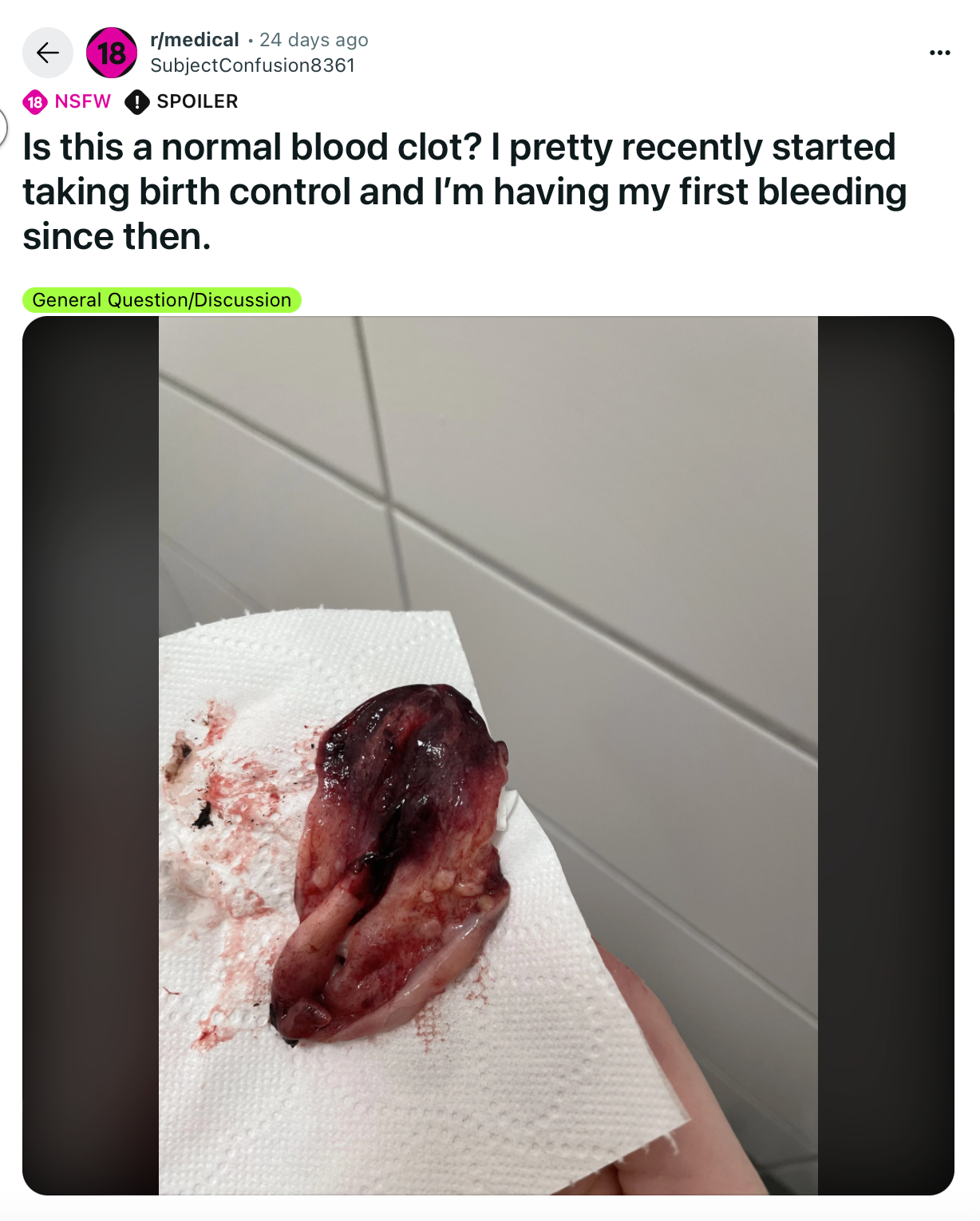
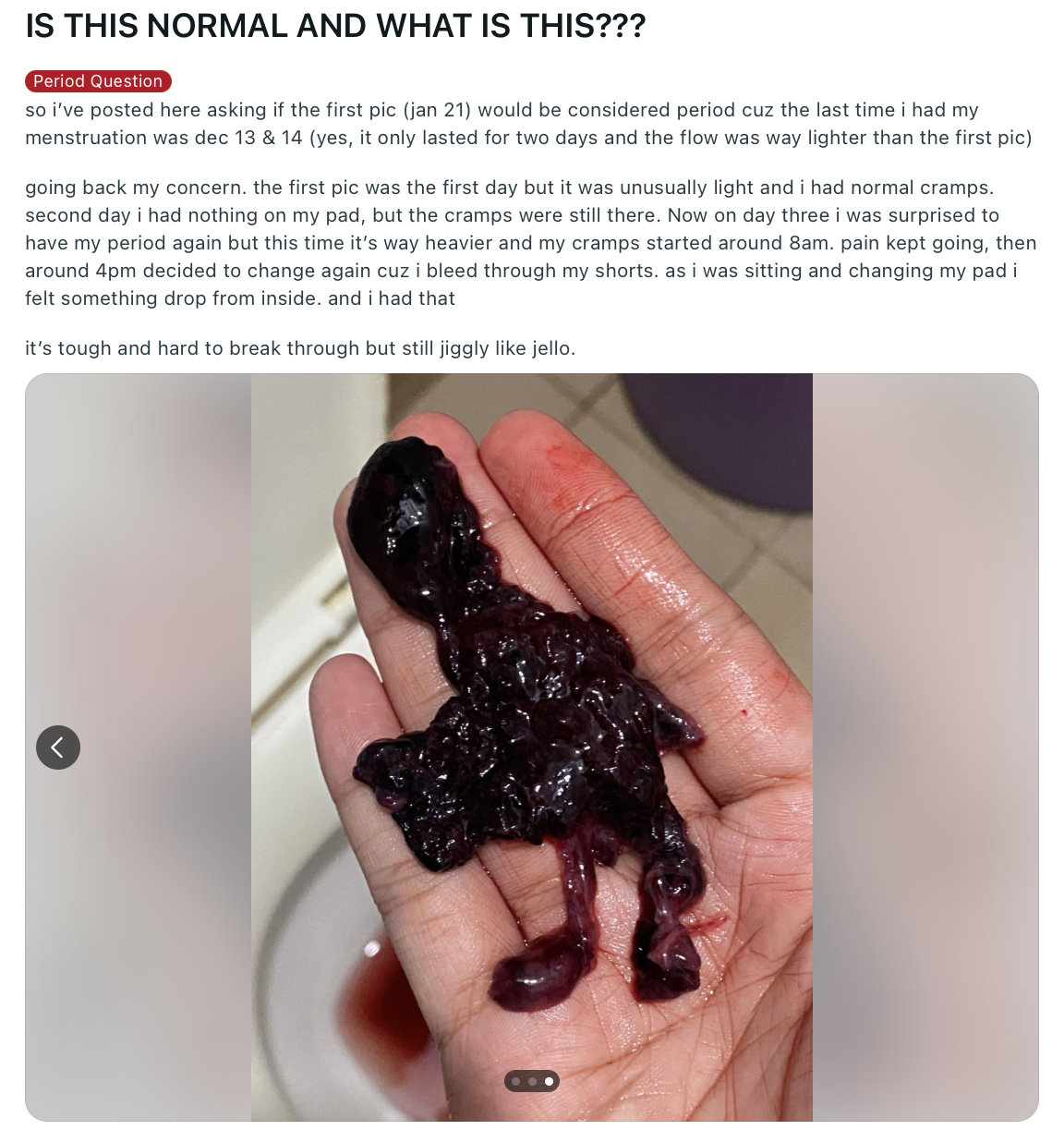
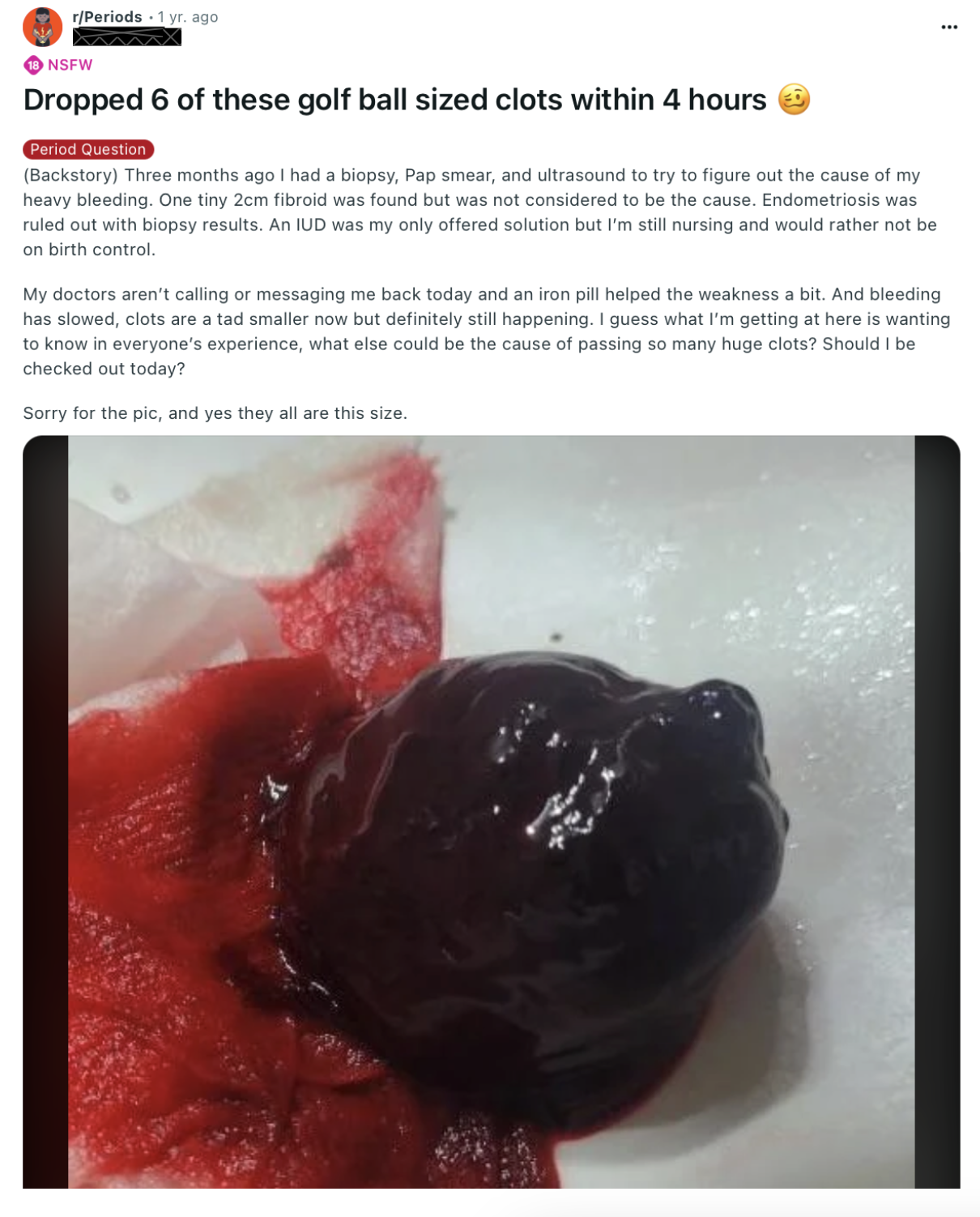
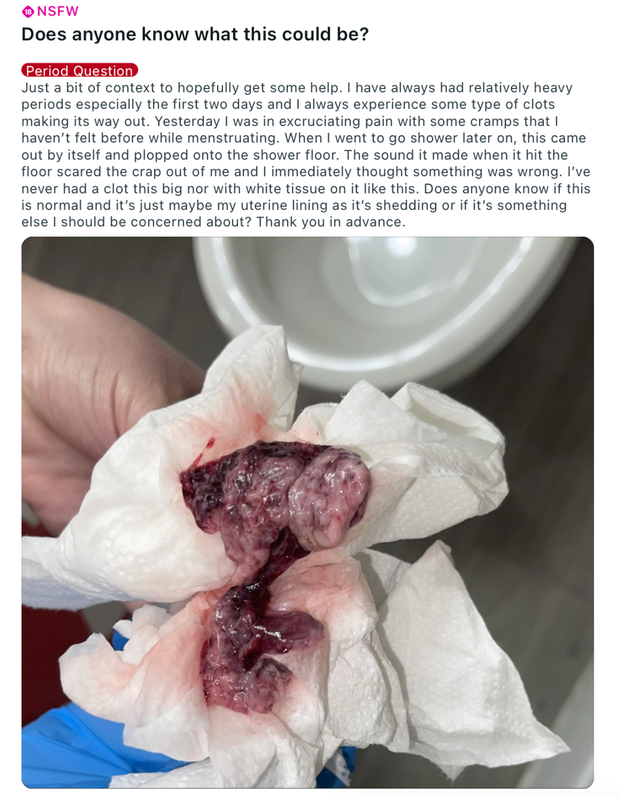
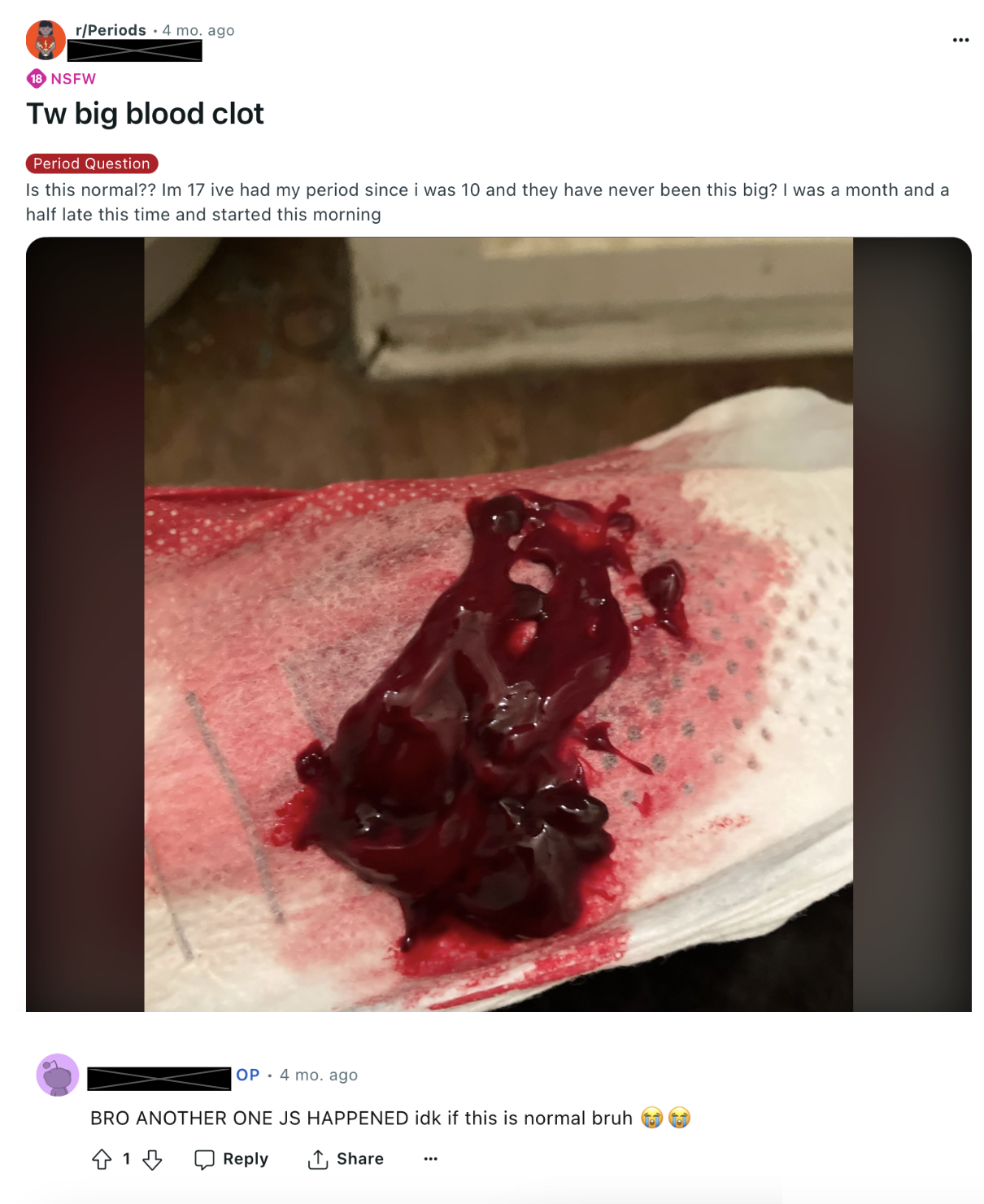
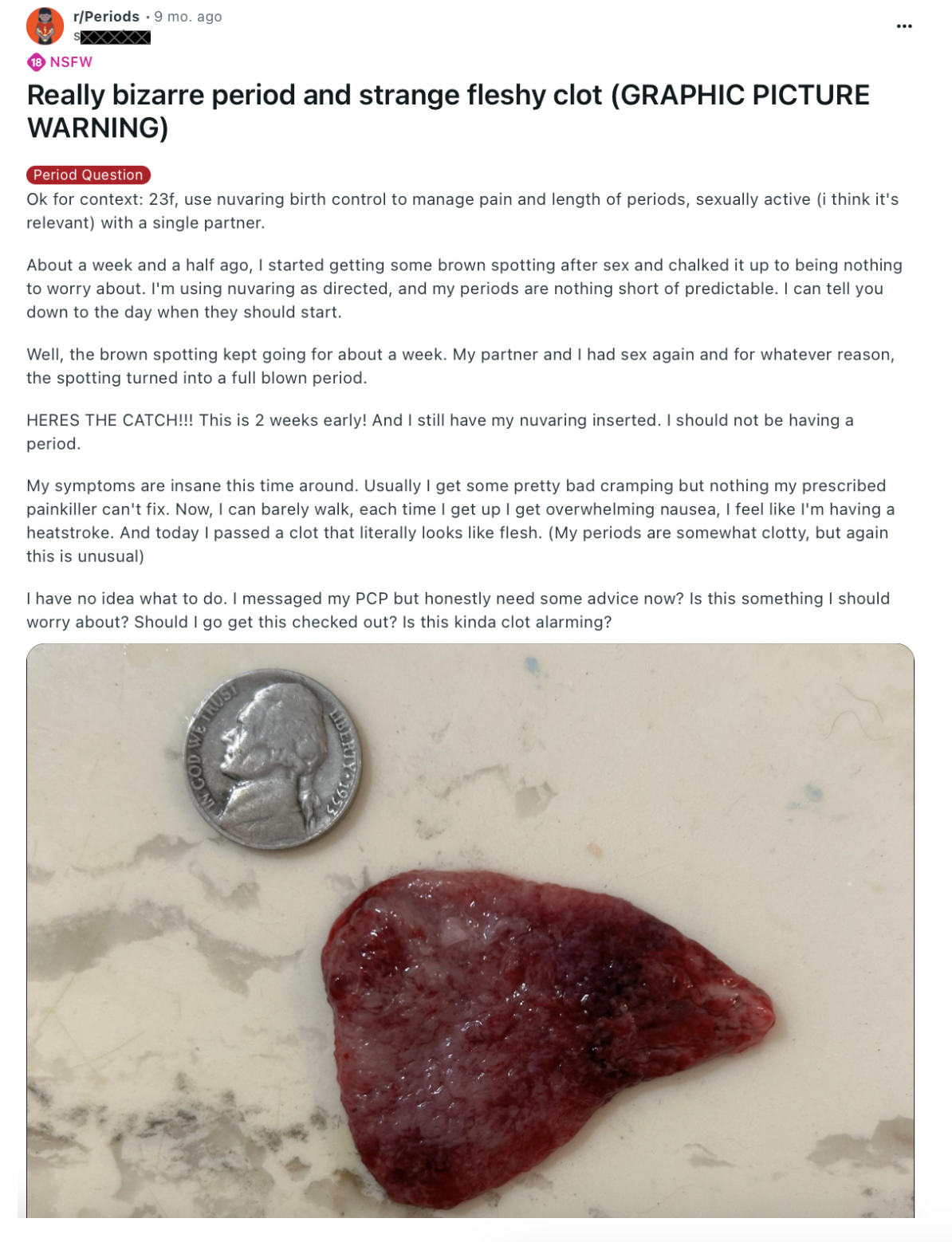
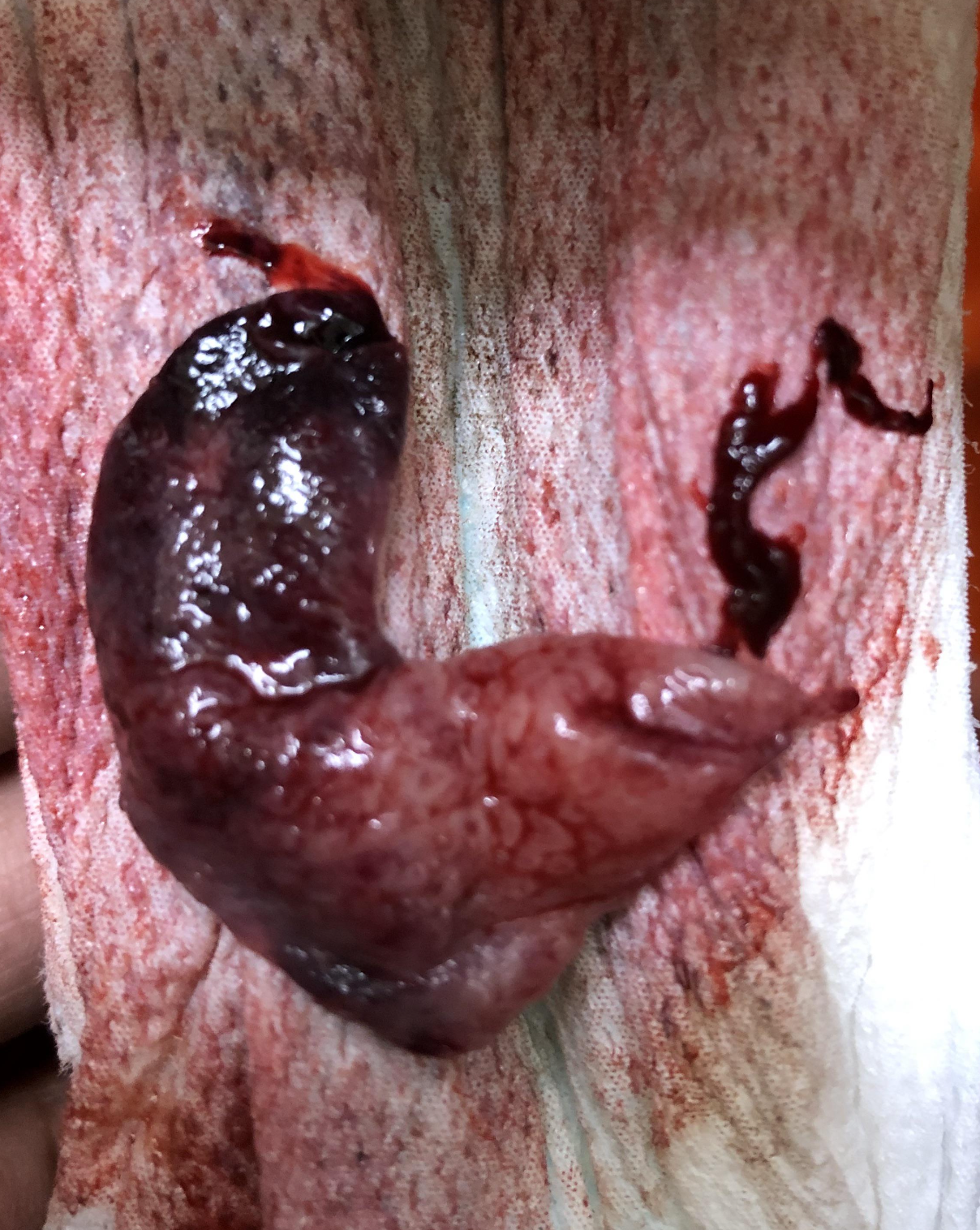
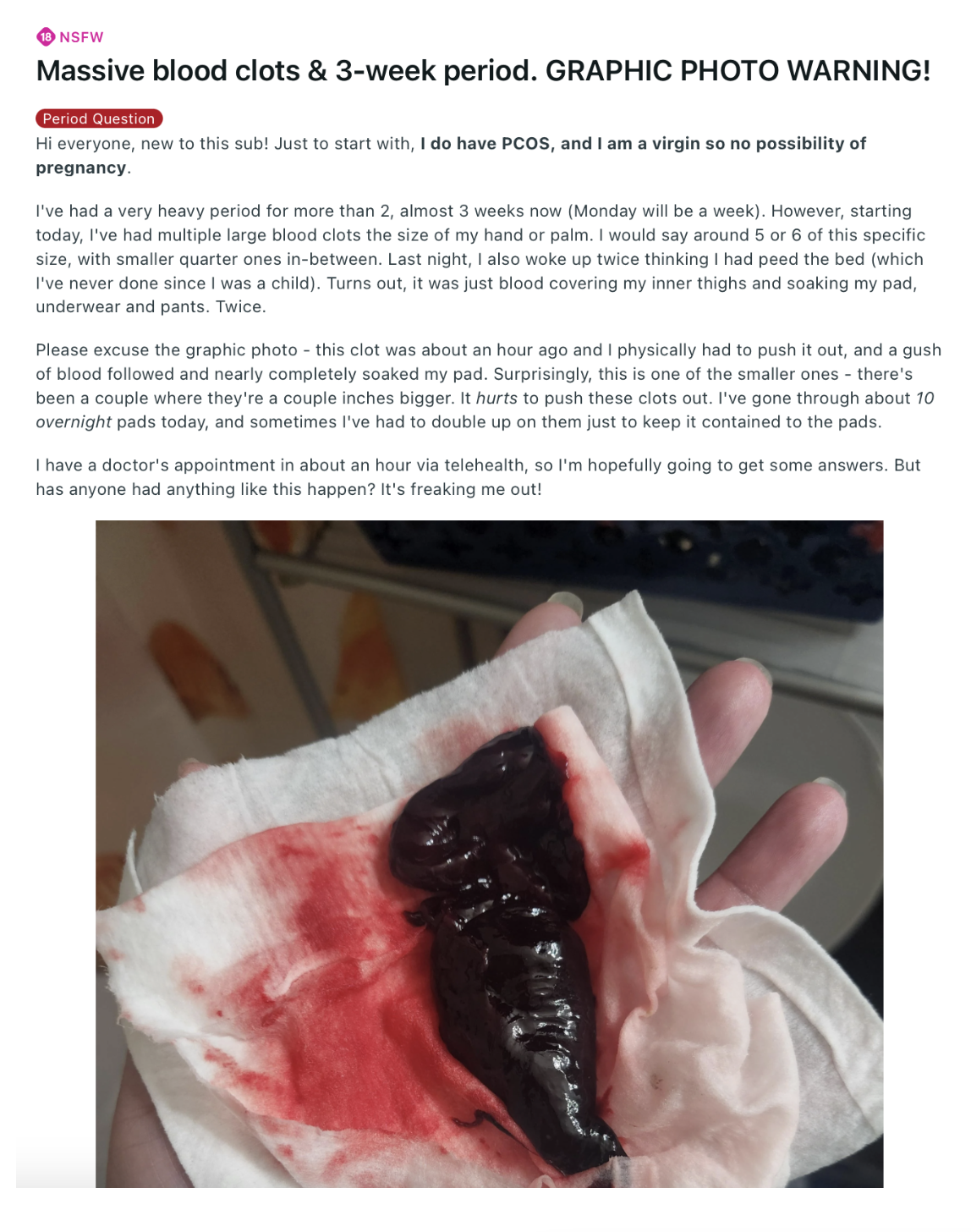
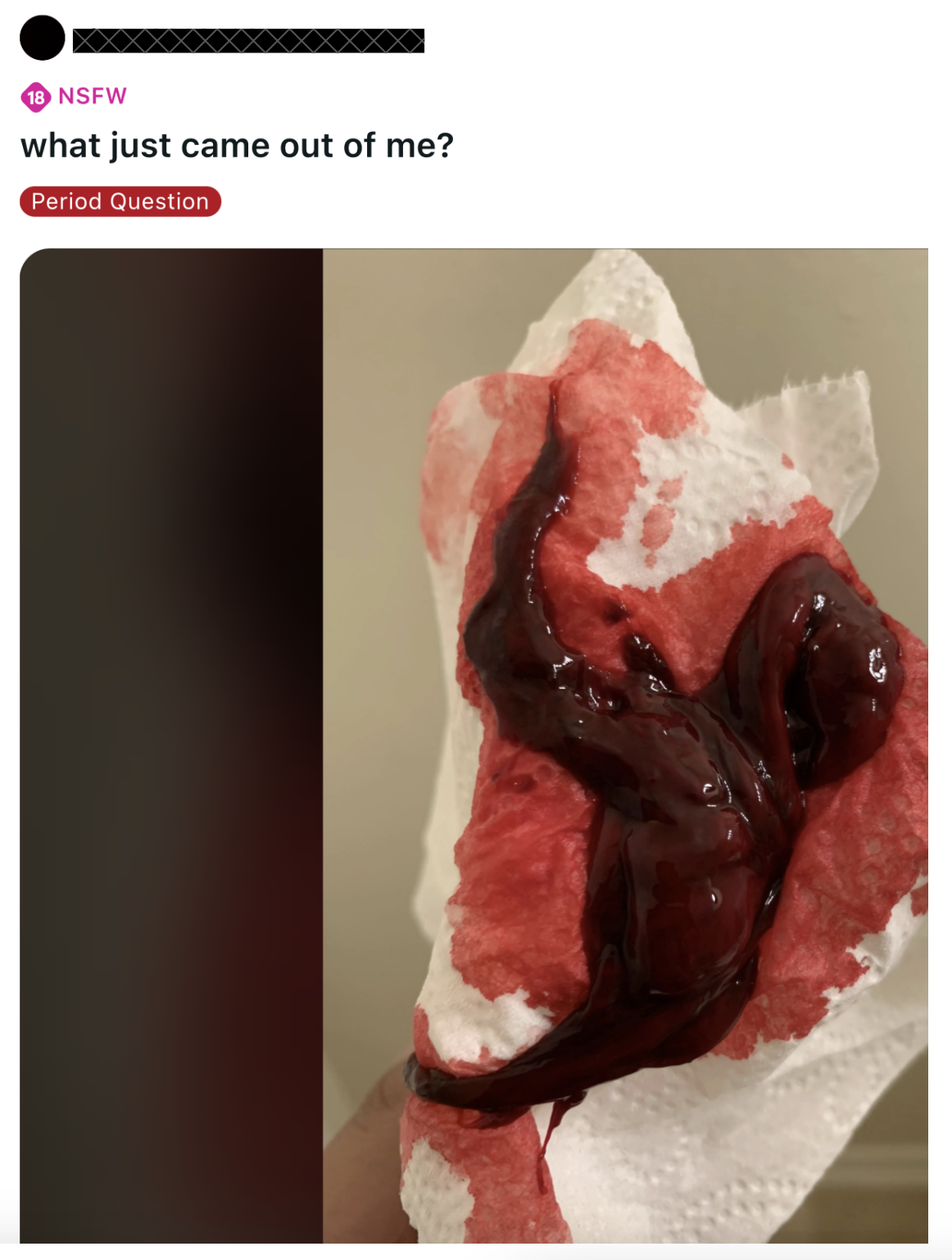
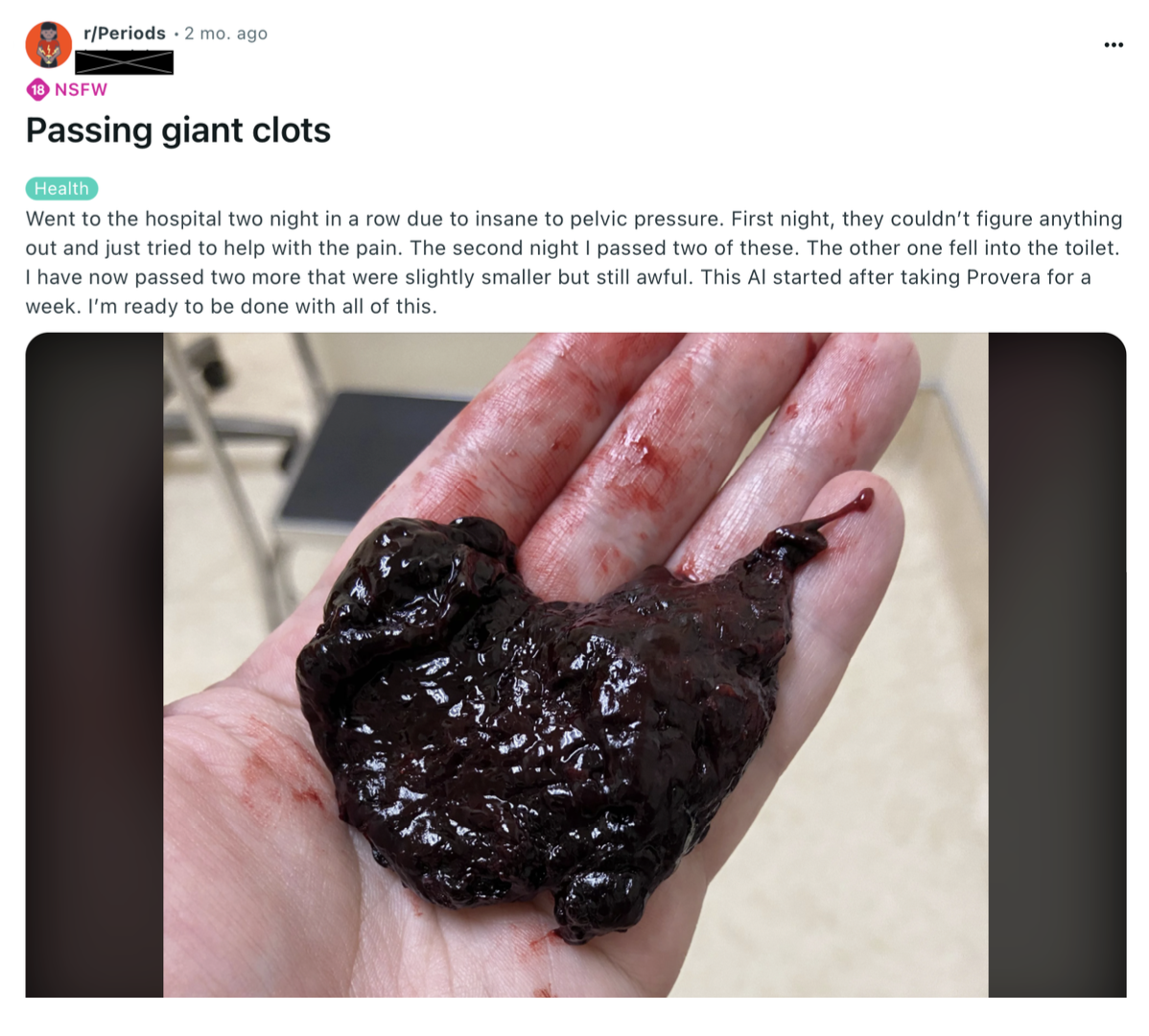
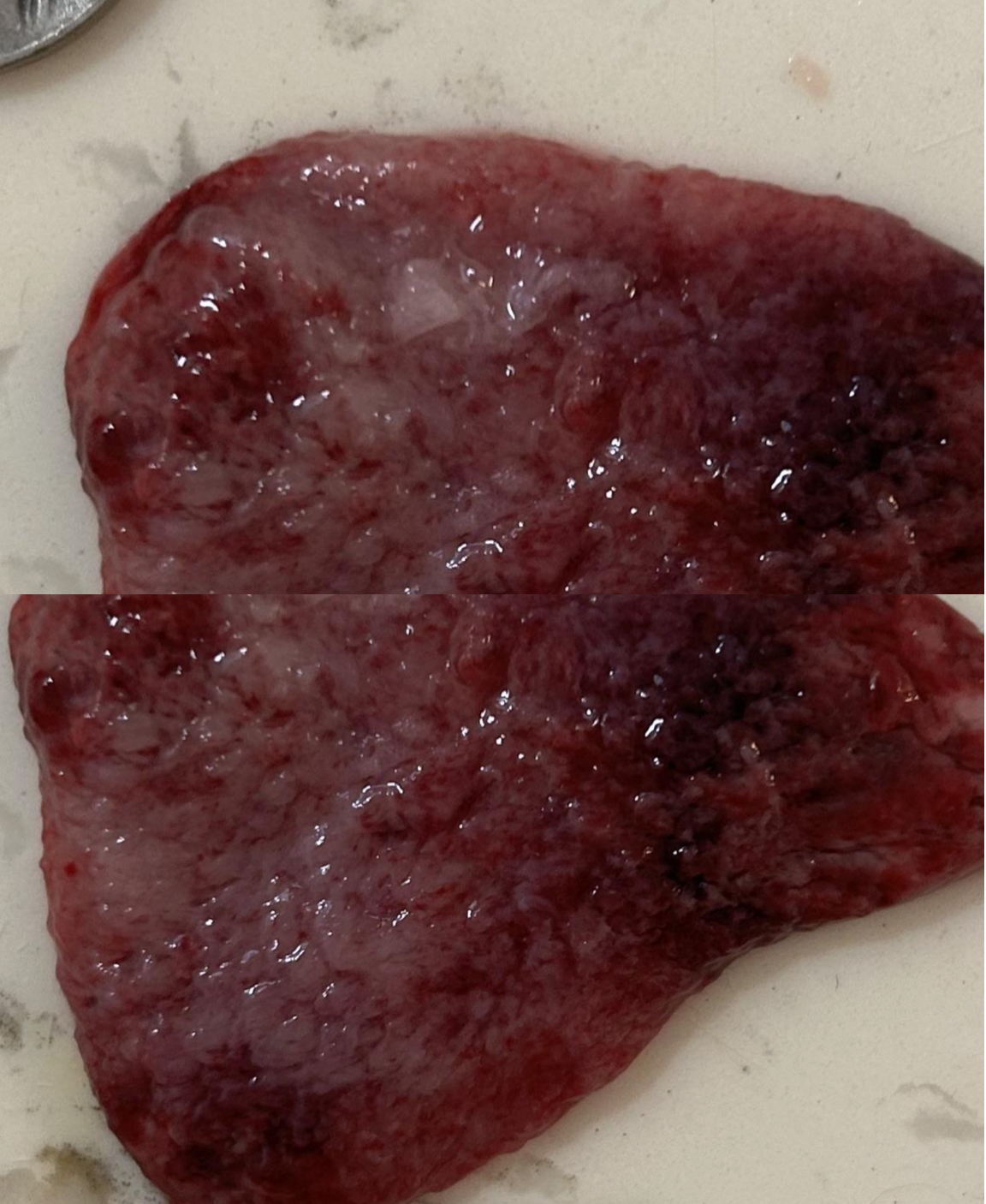
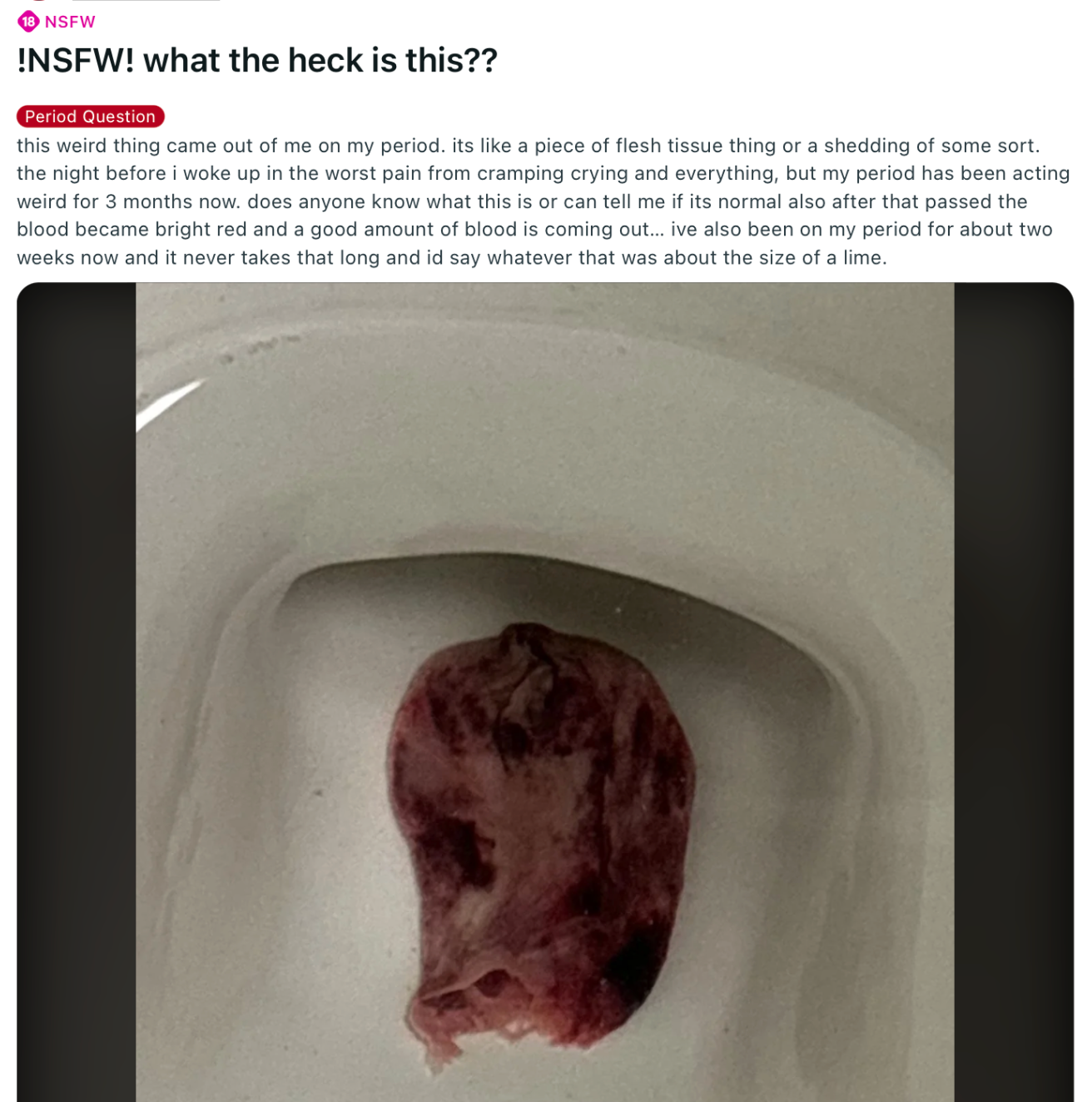
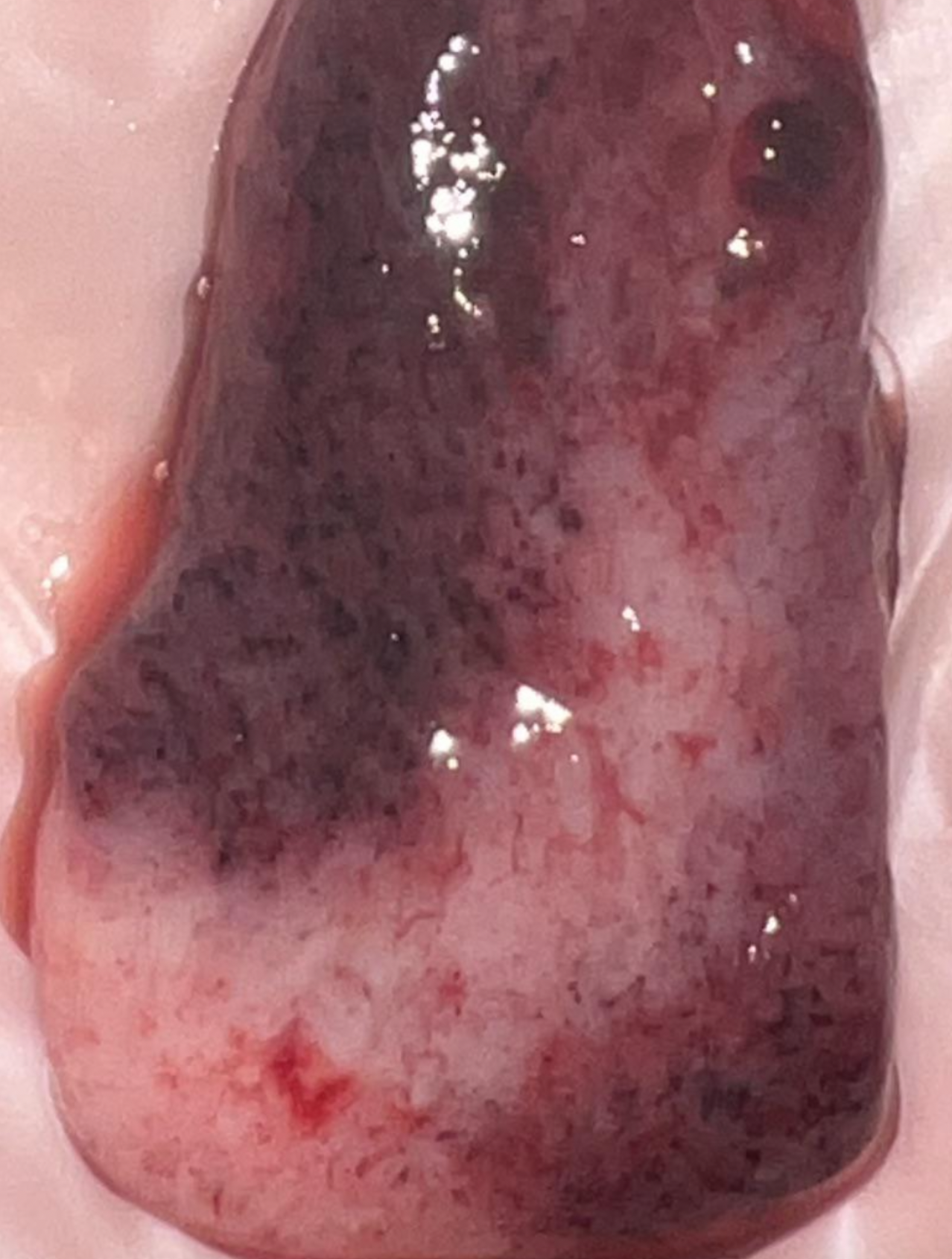
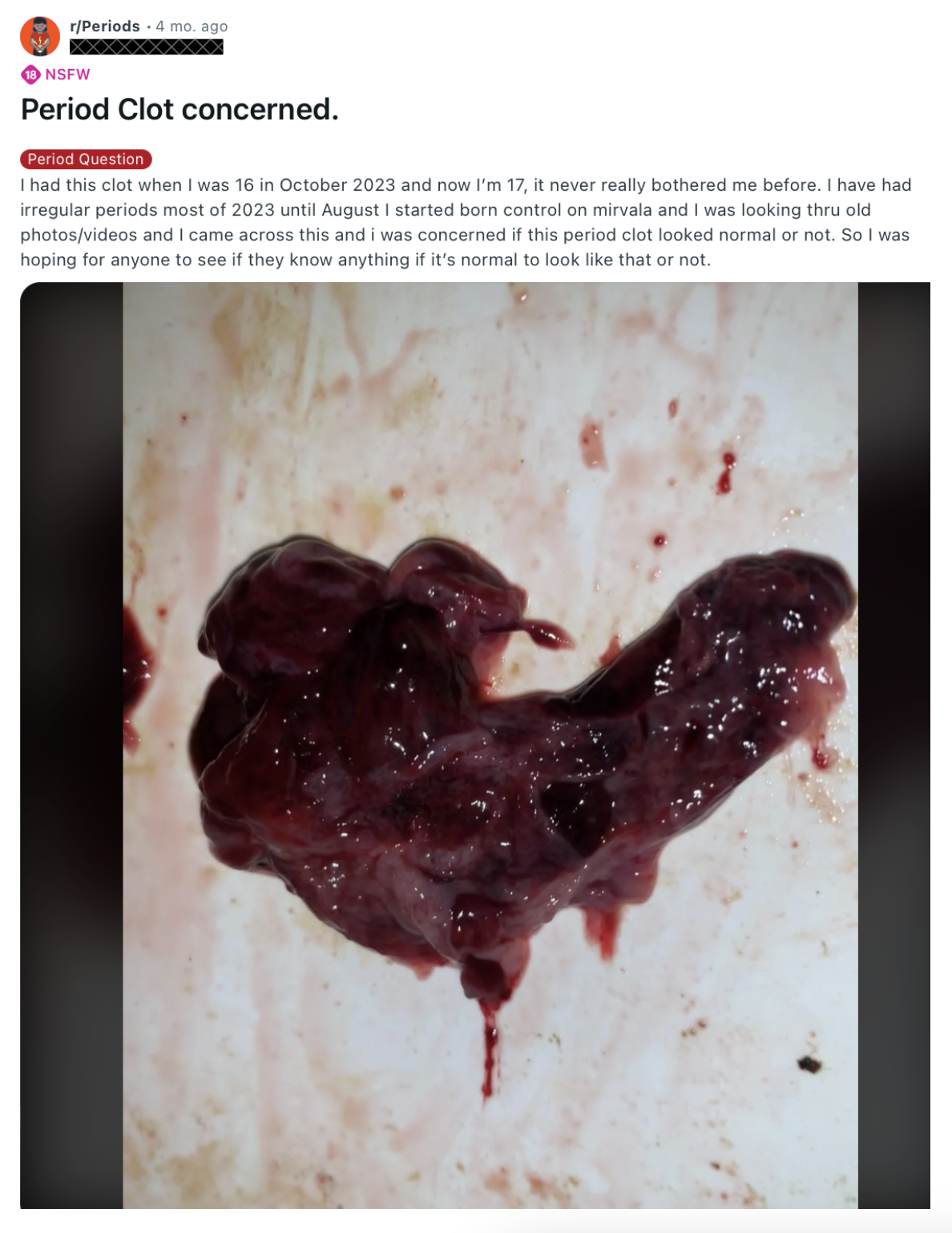
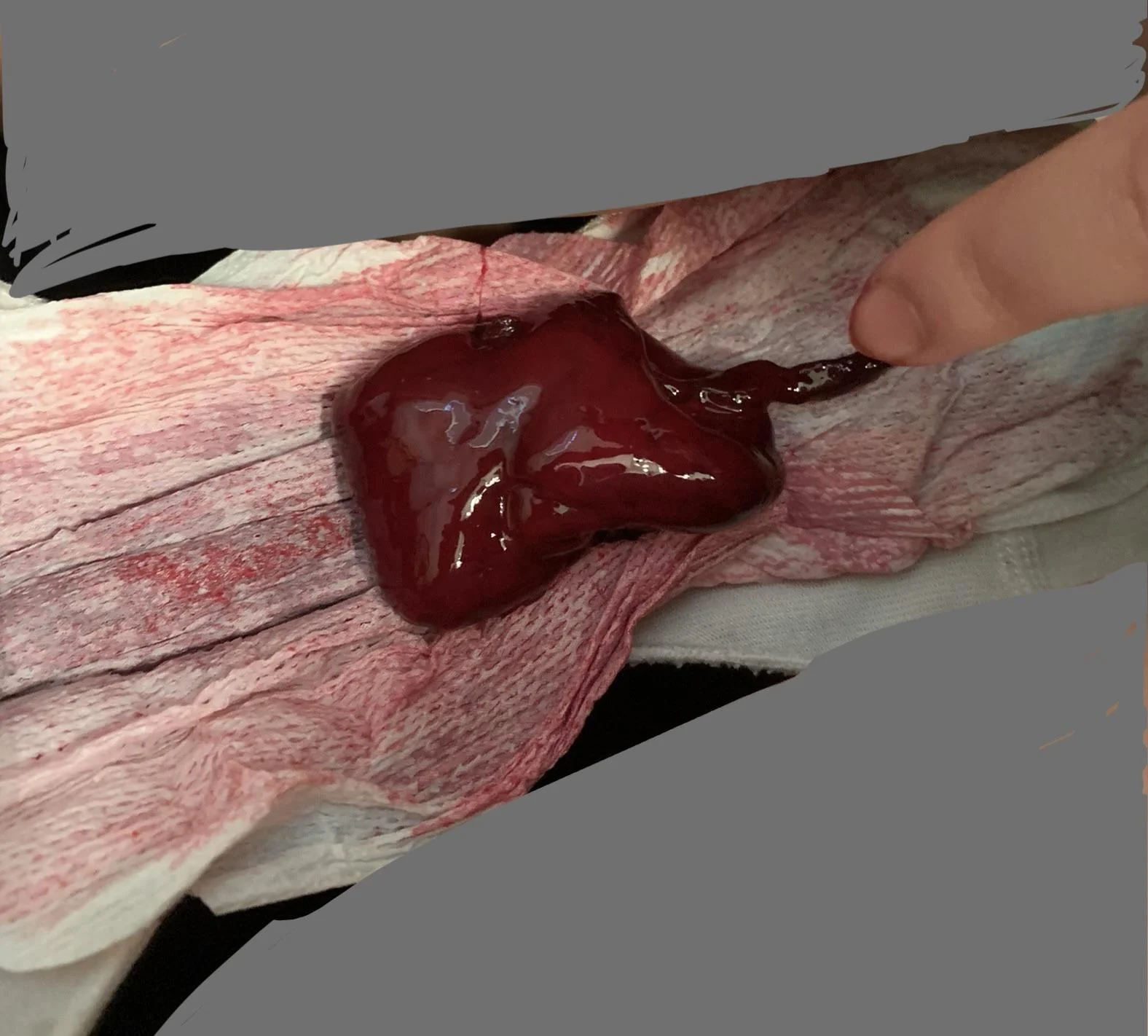
The white to pink tissue is endometrial tissue that has been shed in one piece, retaining the outline of the uterine cavity. In contrast, the dark red blood clots (which can sometimes be very large) result from the build up and coagulation of blood within the uterus.
What's Causing Blood Clots at the Cellular Level
Elevated levels of cytokines (e.g., IL‑6, TNF‑α) can activate vascular endothelial cells to express tissue factor—a key initiator of the coagulation cascade—and reduce fibrinolysis (the process that normally breaks down clots).
Also, the vasoconstriction that normally aids in the menstrual shedding may, if exaggerated, cause blood pooling which can promotes the release of pro-coagulant substances.
As blood exits the small capillaries of the endometrium, the combined effect of endothelial activation and a hypercoagulable environment means that the blood quickly forms fibrin clots rather than remaining a free-flowing fluid.
When the blood isn't able to easily flow out of the capillaries, it causes blood pooling to occur. This reduced blood flow (stasis) allows clotting factors and platelets to further accumulate, leading to a local concentration of inflammatory signals and damage-associated molecules.
With continuous immune-mediated activation, the normal gentle flow that would normally “flush out” menstrual blood is replaced by rapid coagulation. This results in pooled, clotted blood that mix with cellular debris from necrotic endometrial cells to create massive clots.
Membranous Dysmenorrhea: An Underdiagnosed Condition
What's Causing Tissue Clots at the Cellular Level
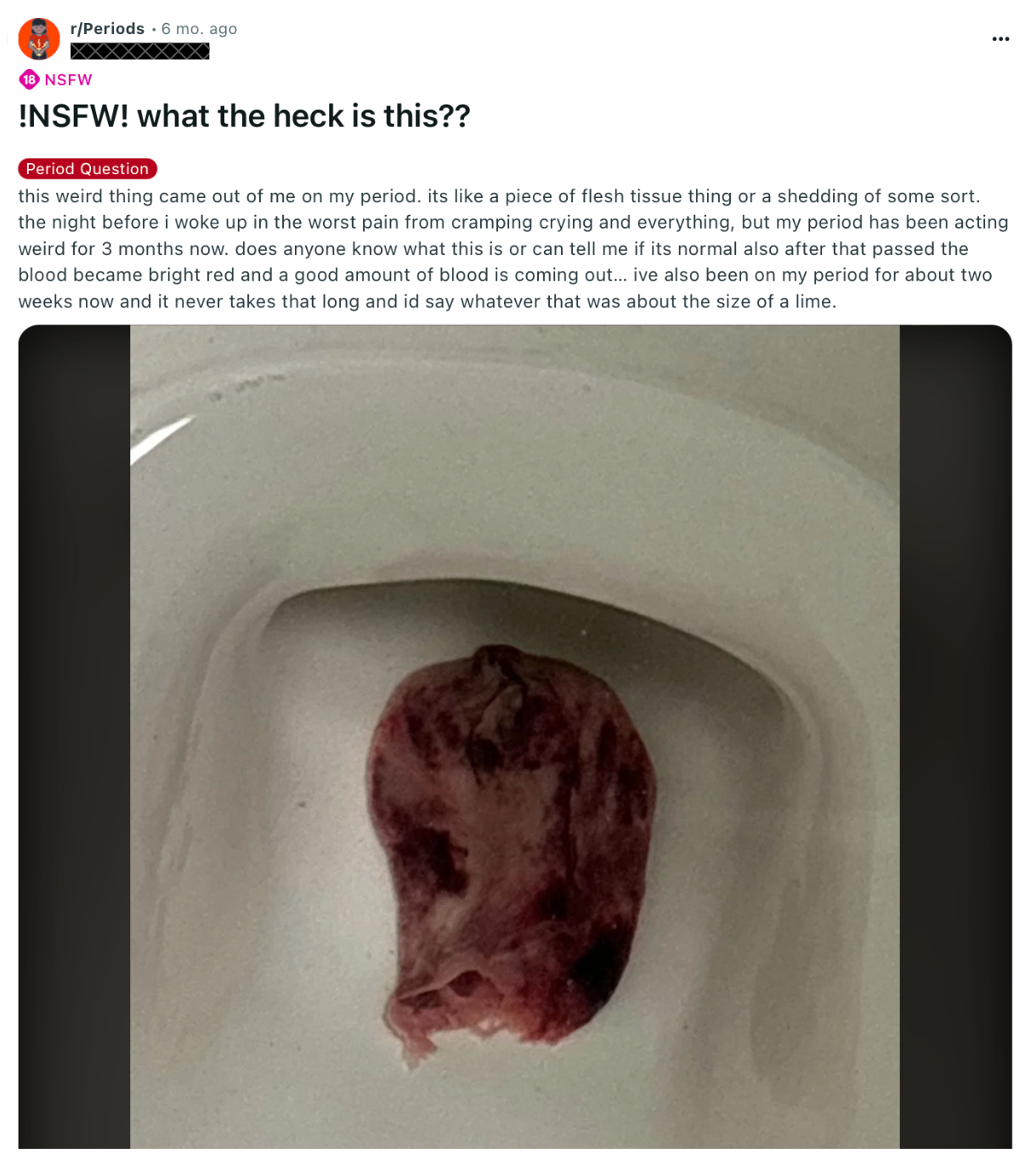
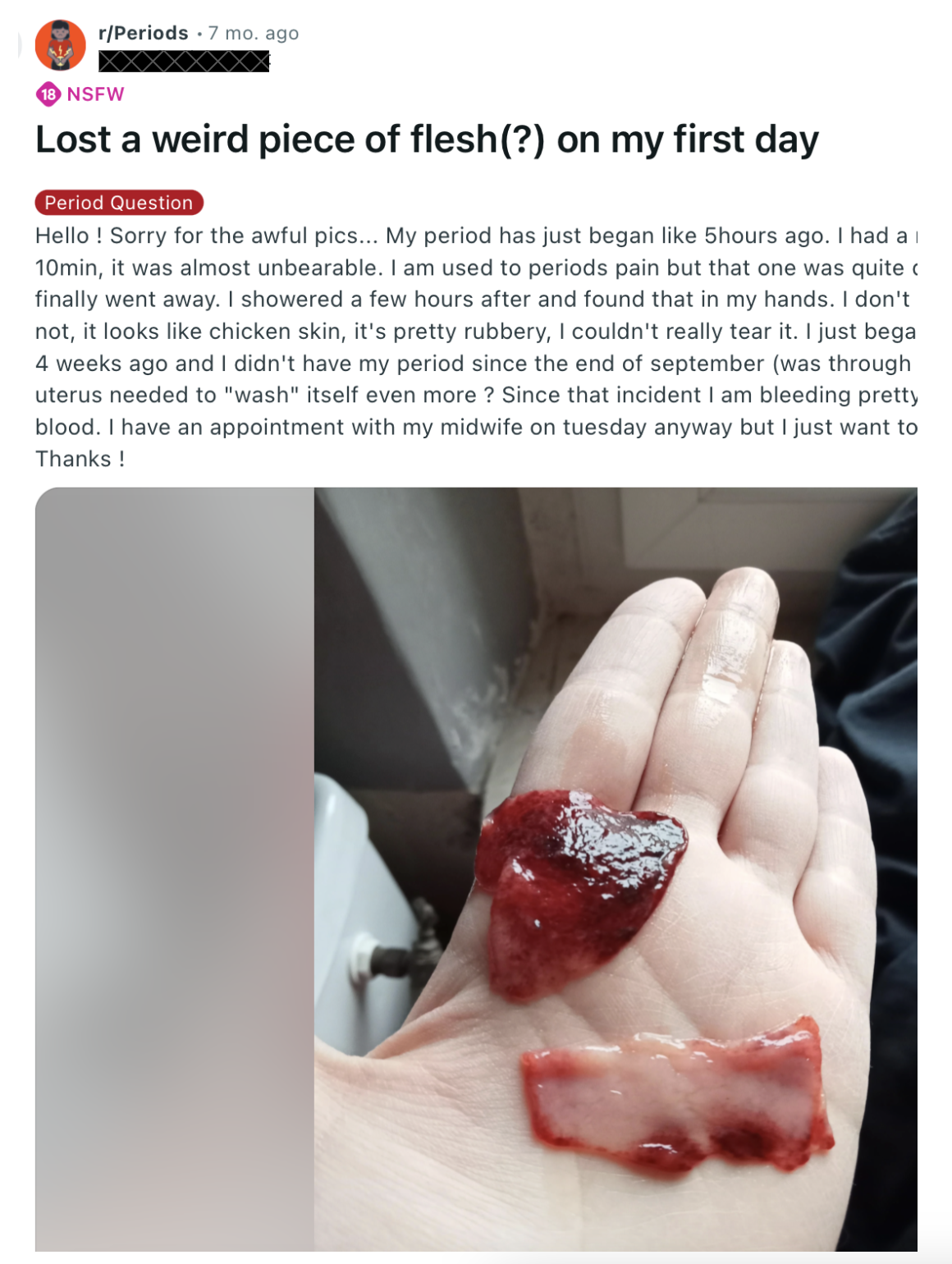
Most women are being told these clots are just decidual casts. The decidua is the thick lining of the uterus that forms as a result of higher than normal levels of progesterone, or an abnormal, overreactive uterine response to progesterone. When progesterone levels abruptly change, the entire thickened lining detaches at once rather than gradually breaking down, leading to the passage of a large, intact tissue cast.
Doctors will tell you they are completely normal and just apart of the menstrual cycle. They will tell you the passing of these massive fleshy pieces of tissue are completely benign, insignificant to over all health, and don't necessarily indicate any intrinsic ovarian pathology.
But how is it that some women go through their entire life without passing these massive fleshy pieces of tissue? If it's normal for so much tissue to build up in the uterus, such that a literal cast of the shape of the uterus is created and then painfully passed, why do "normal" periods just contain blood?
What is the difference between a uterus that passes blood during menstruation, and one that sloughs off a thick layer of tissue? What is driving this uterine tissue to multiply and thicken at such a fast rate? What's driving this exaggerated decidualization of the endometrium?
These tissue casts we are dismissing as normal are actually a sign of membranous dysmenorrhea. They are signals that the endometrium has undergone an unusually strong response to progesterone. So ovaries may be functioning normally in terms of hormone production, but the uterus’s response to the normal hormones is abnormal. But why? What does this mean?
And why on earth would doctors ever think that the best way to treat abnormal responses to progesterone in the uterus would be to add more progesterone in the form of birth control? How does that even make sense?
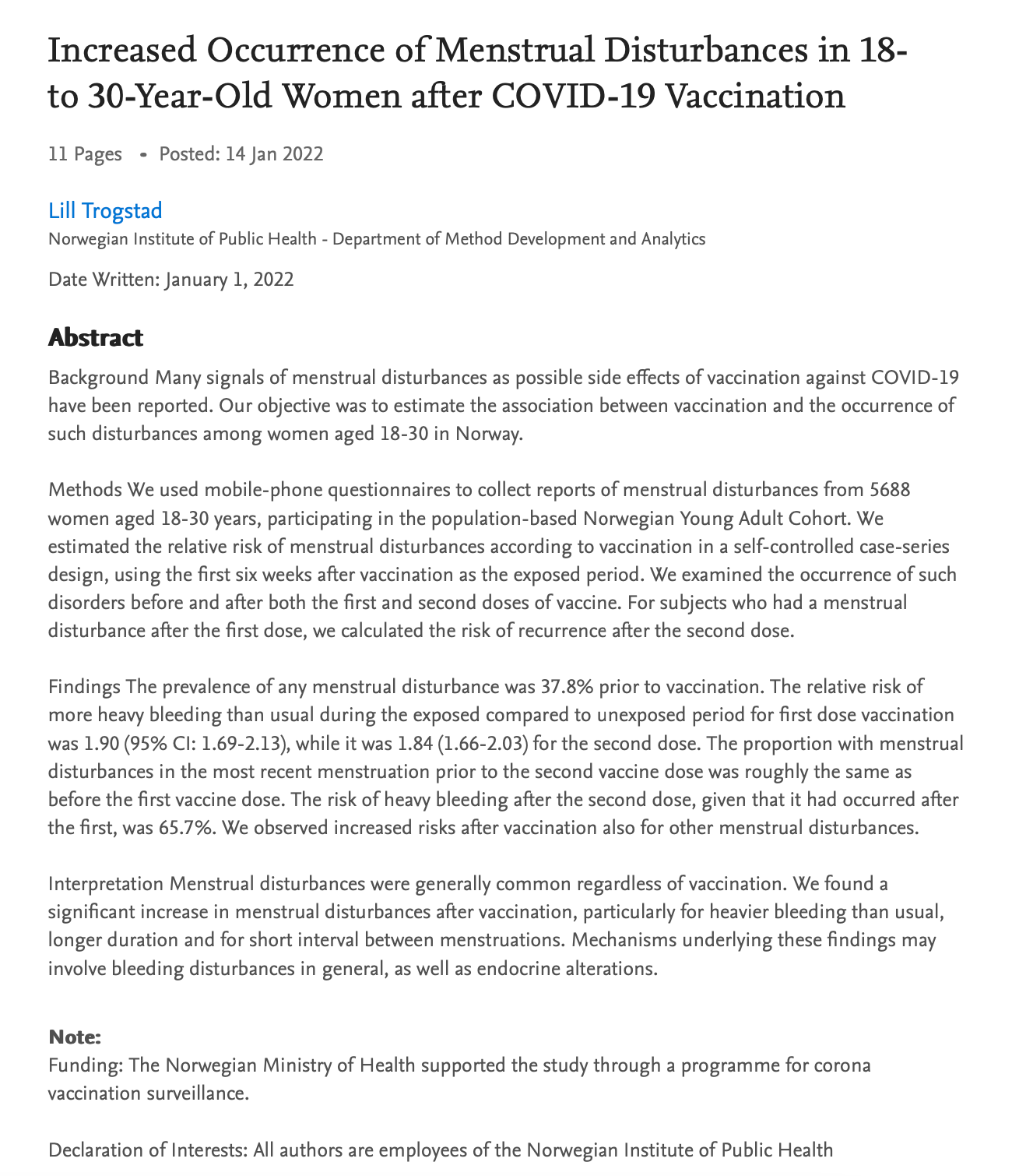
How could the vaccine play a part?
Vaccines, particularly mRNA vaccines, are designed to stimulate an intense immune response. In doing so, they temporarily increase the production of cytokines (immune signaling molecules). These inflammatory cytokines (e.g., IL‑6, TNF‑α) can cause vascular endothelial cells to:
- Upregulate tissue factor expression on endothelial surfaces.
- Downregulate fibrinolytic activity.
This leads to a disruption of the uterine environment that can have a cascade effect on the uterus' ability to flush out dead cells and reform new cell lining.
If uterine cells begin to build up or act abnormally, it could lead to an autoimmune response to the uterine cells. The body’s immune system could then mistakenly targets self-antigens on uterine cells (or on the vascular endothelium of the endometrium), leading to:
- Chronic local inflammation.
- Direct endothelial cell damage.
Both of these effects promote abnormal coagulation by exposing subendothelial tissue and triggering clotting cascades.
In chronic autoimmune states, persistent antibody production leads to the formation of immune complexes that deposit in small blood vessels. These deposits, along with complement activation, damage or activate endothelial cells lining the capillaries of the endometrium.
Damaged endothelial cells upregulate pro‐coagulant molecules (for example, tissue factor) while reducing the production of natural anticoagulants. Chronic immune activation may also lead to the production of antibodies (e.g., anti-phospholipid antibodies) that directly enhance platelet activation and coagulation.
Chronic production of antibodies can also lead to hormonal imbalances that affect the endometrial response. The menstrual cycle is tightly regulated by a network of hormonal and immune signals, so an abnormal shedding pattern can be a signal of a broader hormonal or inflammatory dysregulation in the body.
Throughout the cycle, the hypothalamus releases gonadotropin-releasing hormone (GnRH) in a pulsatile manner, which drives the pituitary to secrete follicle-stimulating hormone (FSH) and luteinizing hormone (LH). These, in turn, stimulate the ovaries to produce estrogen and progesterone.
So the systematic immune activation triggered by vaccines can affect both the hypothalamic–pituitary–ovarian (HPO) axis and the local uterine immune responses.
Why is Birth Control A Terrible Idea for Treating Any of These Symptoms?
Progestins in birth control cause an overly strong decidualization (differentiation) of the endometrial stromal cells. Normally, the endometrium builds up and is gradually shed, but if the endometrial cells are hyper-responsive, they may overgrow and form an unusually thick lining - hyperdecidualization.
When this hyperthickened lining eventually breaks down, it may not be fragmented into small pieces that are easily flushed out. Instead, the entire layer can detach as a cohesive “cast,” sometimes accompanied by heavy, clotted blood.
Exogenous hormones can also affect the balance between pro-coagulant and anti-coagulant factors within the uterus. Under normal conditions, small ruptures in the endometrial capillaries produce just enough fibrin to stop bleeding temporarily without forming large clots. However, if hormonal stimulation is excessive, the local release of inflammatory cytokines and tissue factor may be amplified. This creates a microenvironment where the blood rapidly coagulates rather than flows out smoothly.
If uterine contractions (which normally help expel menstrual flow) are impaired or if there is pooling of blood, even a slight shift toward a pro-coagulant state can result in blood quickly forming large clots. These clots, rather than being broken down and washed away, accumulate and may combine with overgrown endometrial tissue.
In the case of massive clots or tissue, endometrial cells are already under stress and disfunction. Additional progestin further stimulates a dysregulated immune response and enhances endothelial activation leading to tissue build up or clotting.
Decidual Casts: Signals of Hyperprogesteronism
What does this look like?





















































Discussion