

What is Leukemia?
Leukemia is caused by complete dysregulation of immune cells, allowing them to proliferate throughout the body and wreak immense damage on healthy cells.
What is so strange about leukemia is that the immune cell's primary role in the body is to detect and eliminate cancerous cells before they can develop into full-blown malignancies – not to become cancerous themselves. Most cancers arise in solid organs, such as the lungs, liver, or skin. It was historically thought that immune cells could not be prone to cancer, since their primary function is to destroy mutated or infected cells.
But over the past 25 years, the rise of immune-related cancers like leukemia, lymphoma, and multiple myeloma suggests that something has fundamentally altered immune system function, leading to unchecked proliferation of white blood cells.
It's interesting that our country has one the highest rates of leukemia in children under 10 years old, with 1 in 20,408 children in America under 10 receiving a leukemia diagnosis. In comparison, Sudan only has 1 in 106,383 children under ten receive a cancer diagnosis.
It might not be a surprise that Sudan also doesn't require vaccination at birth and has no explicit national policy mandating them as a prerequisite for school enrollment. The recommended vaccine schedule also has 15 fewer shots than America does for children 10 years and younger.
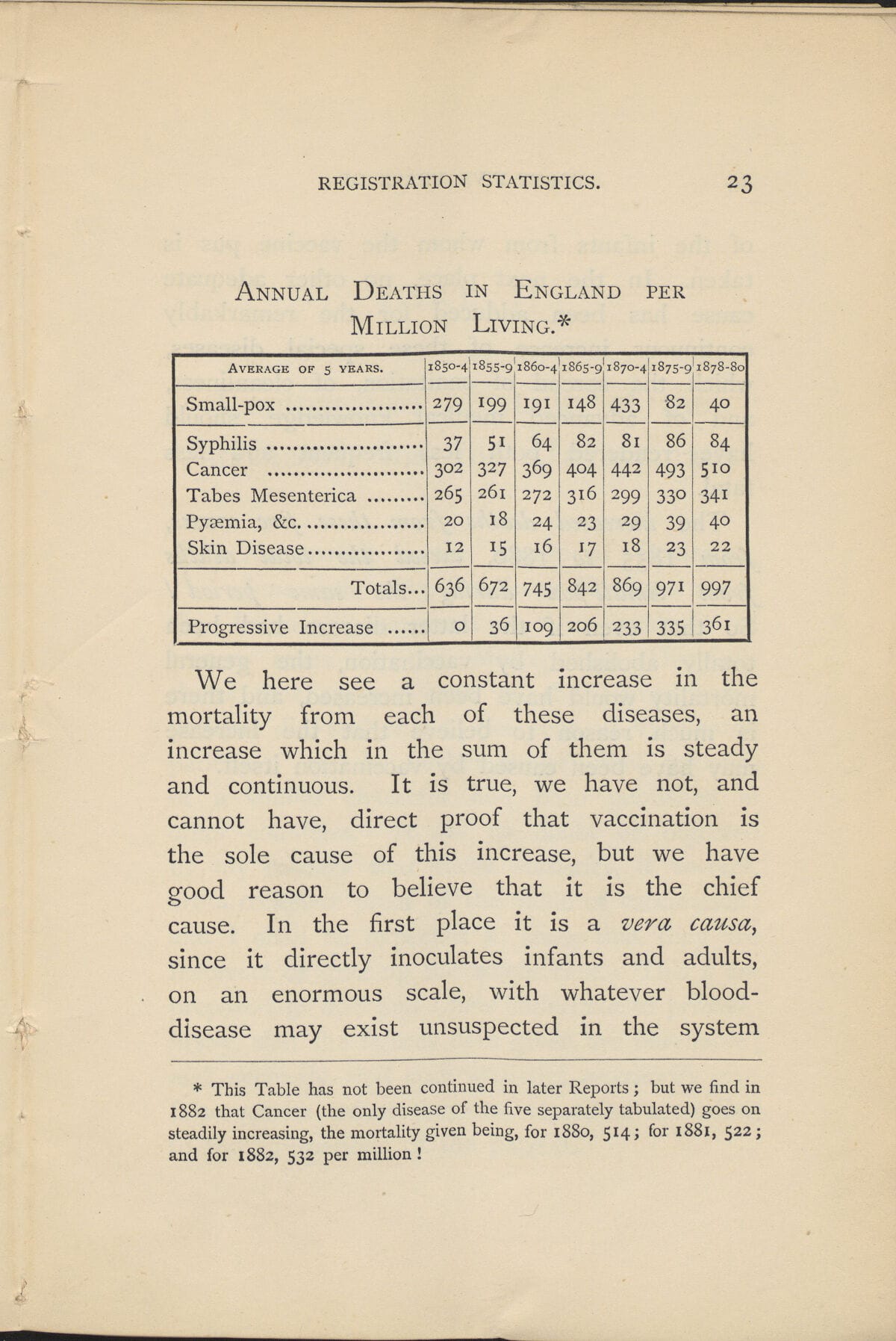
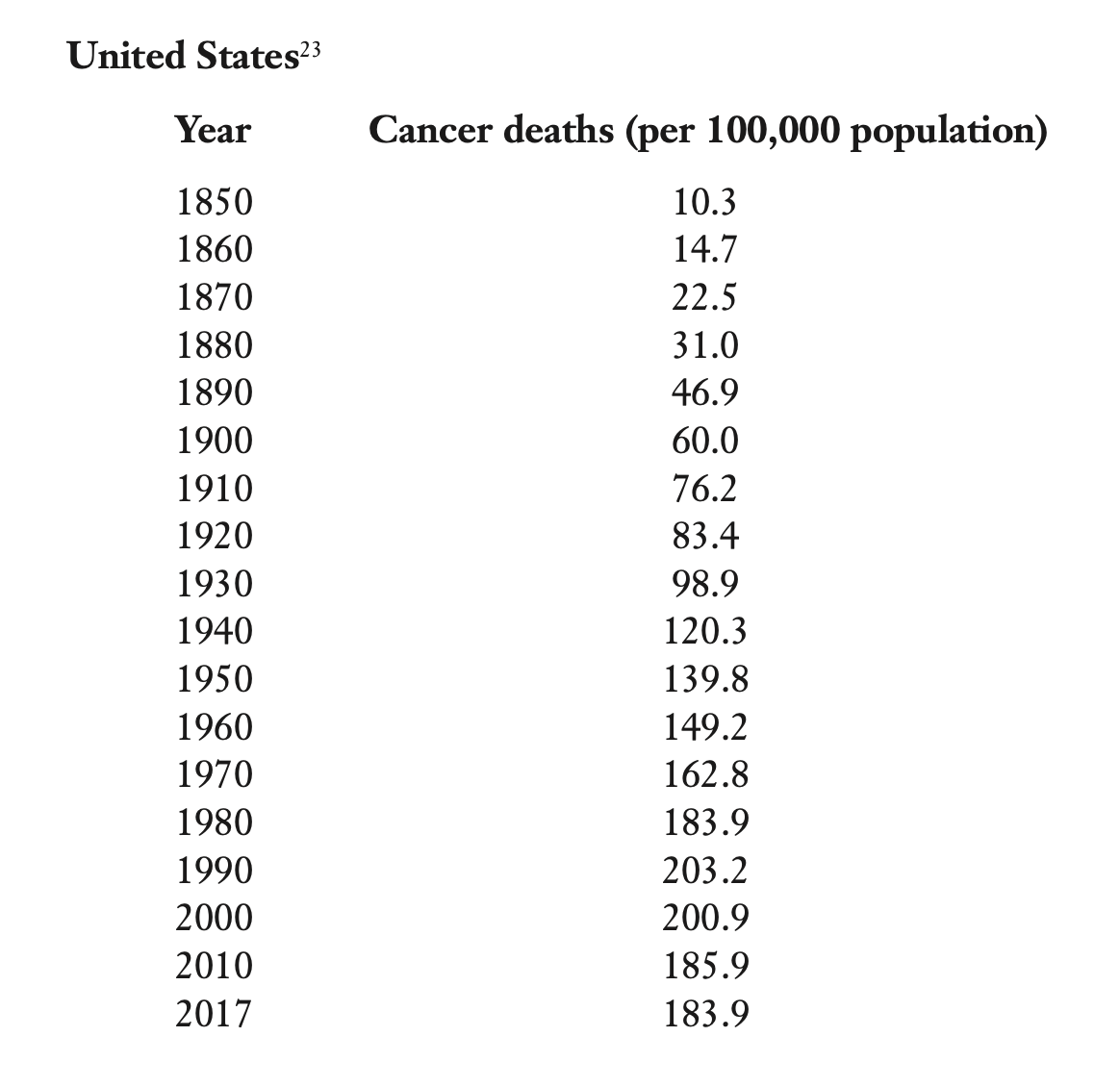
Leukemia Did Not Exist Before Vaccines
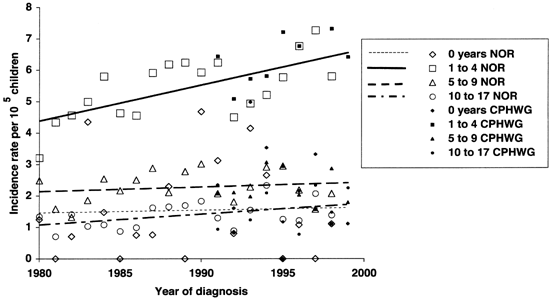
Leukemia was first described in 1845 by Rudolf Virchow and John Hughes, just 60 years after vaccination was introduced to society. Since then, the incidence of leukemia has increased dramatically, particularly in children.
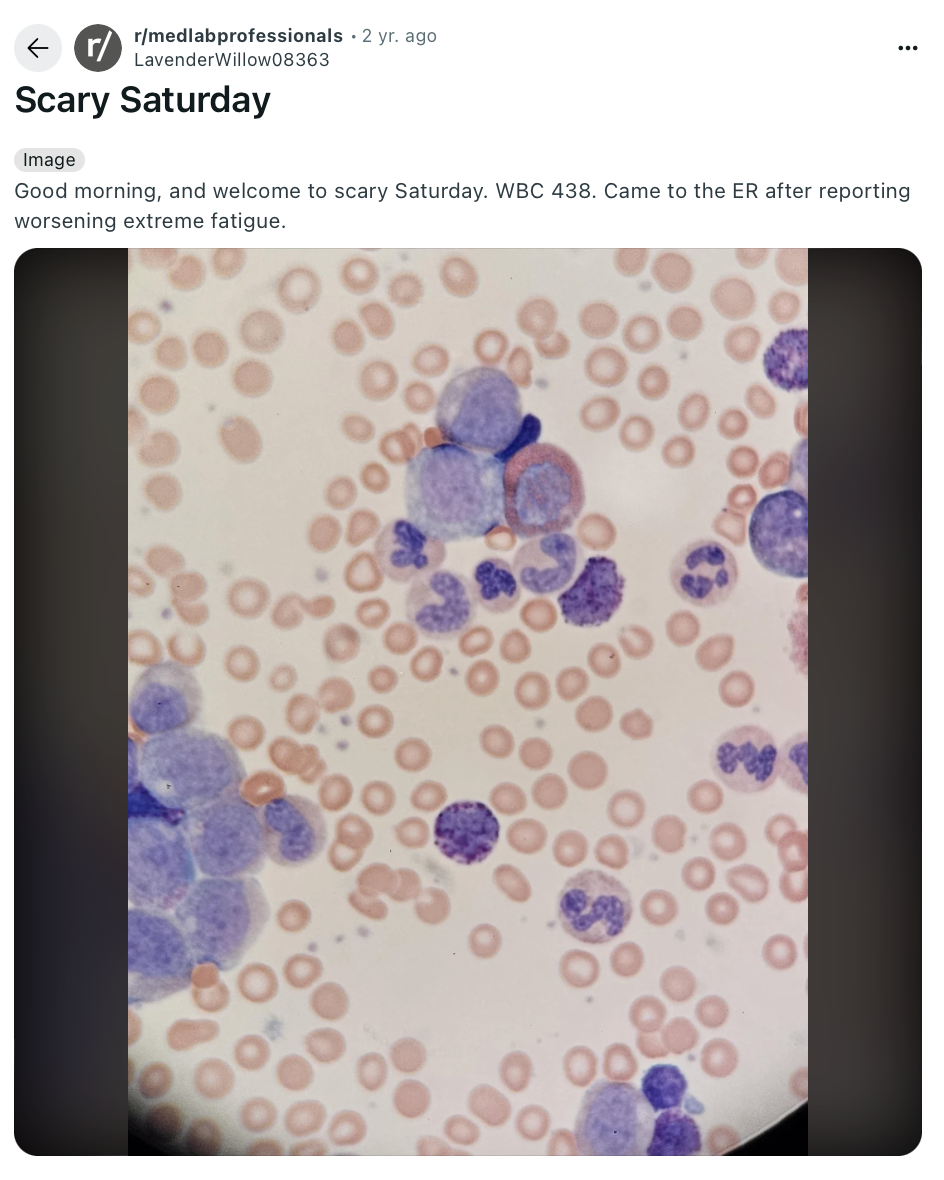
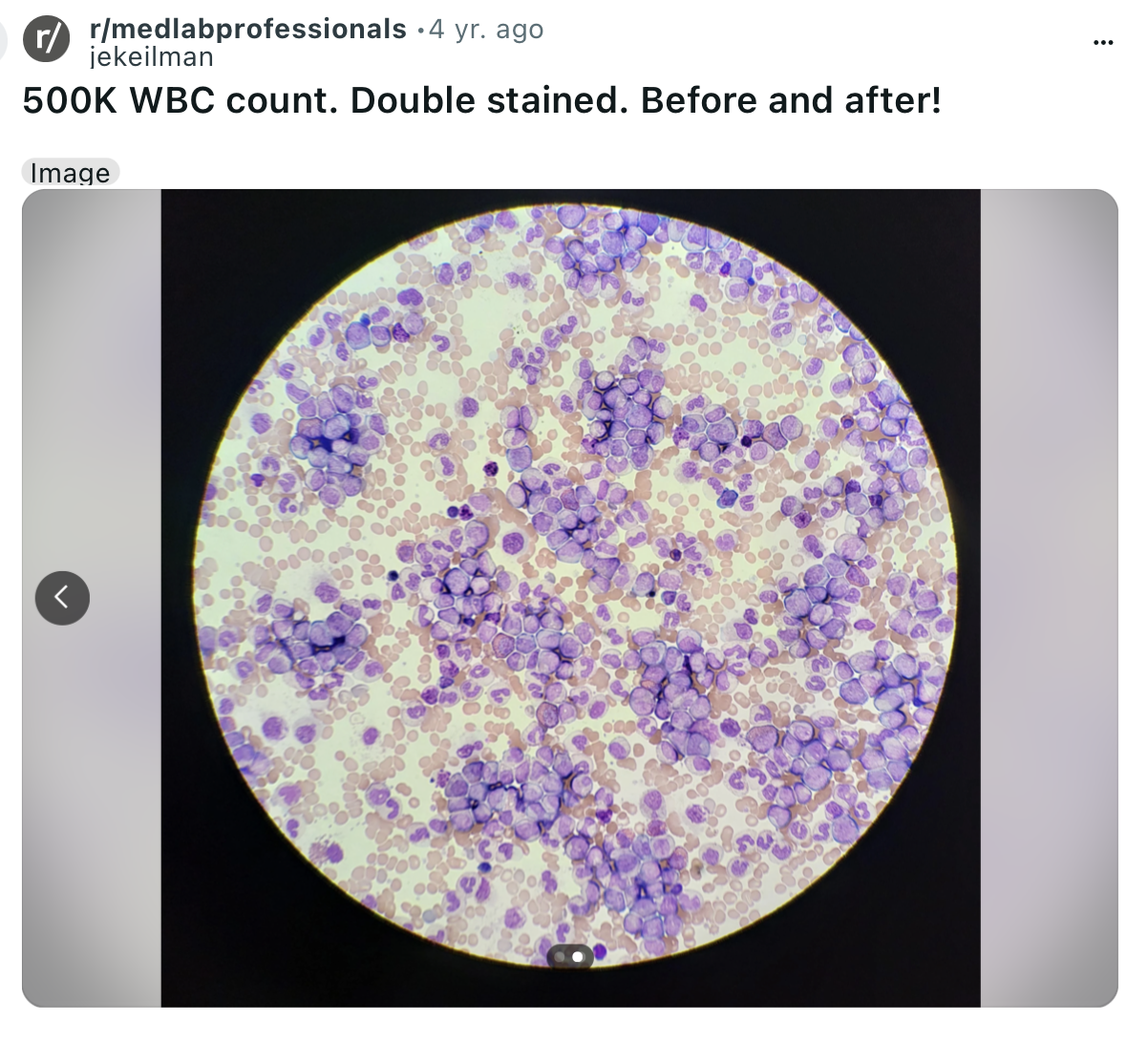
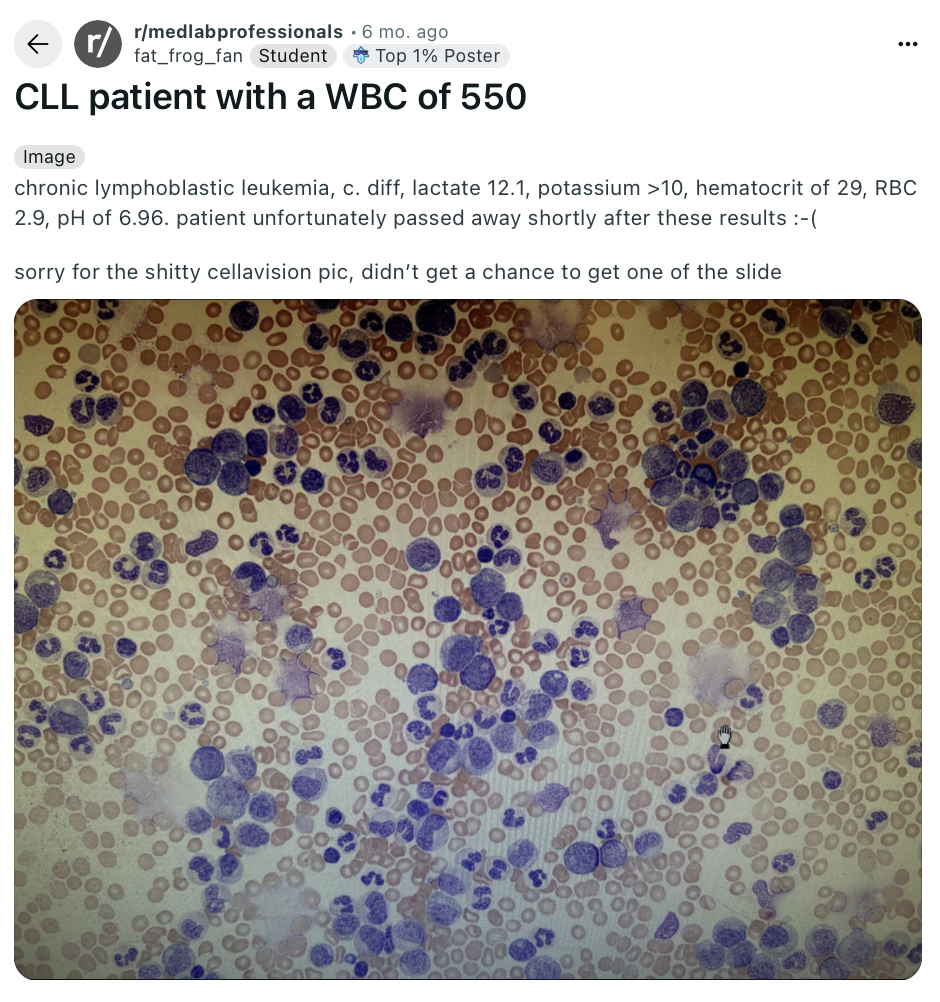
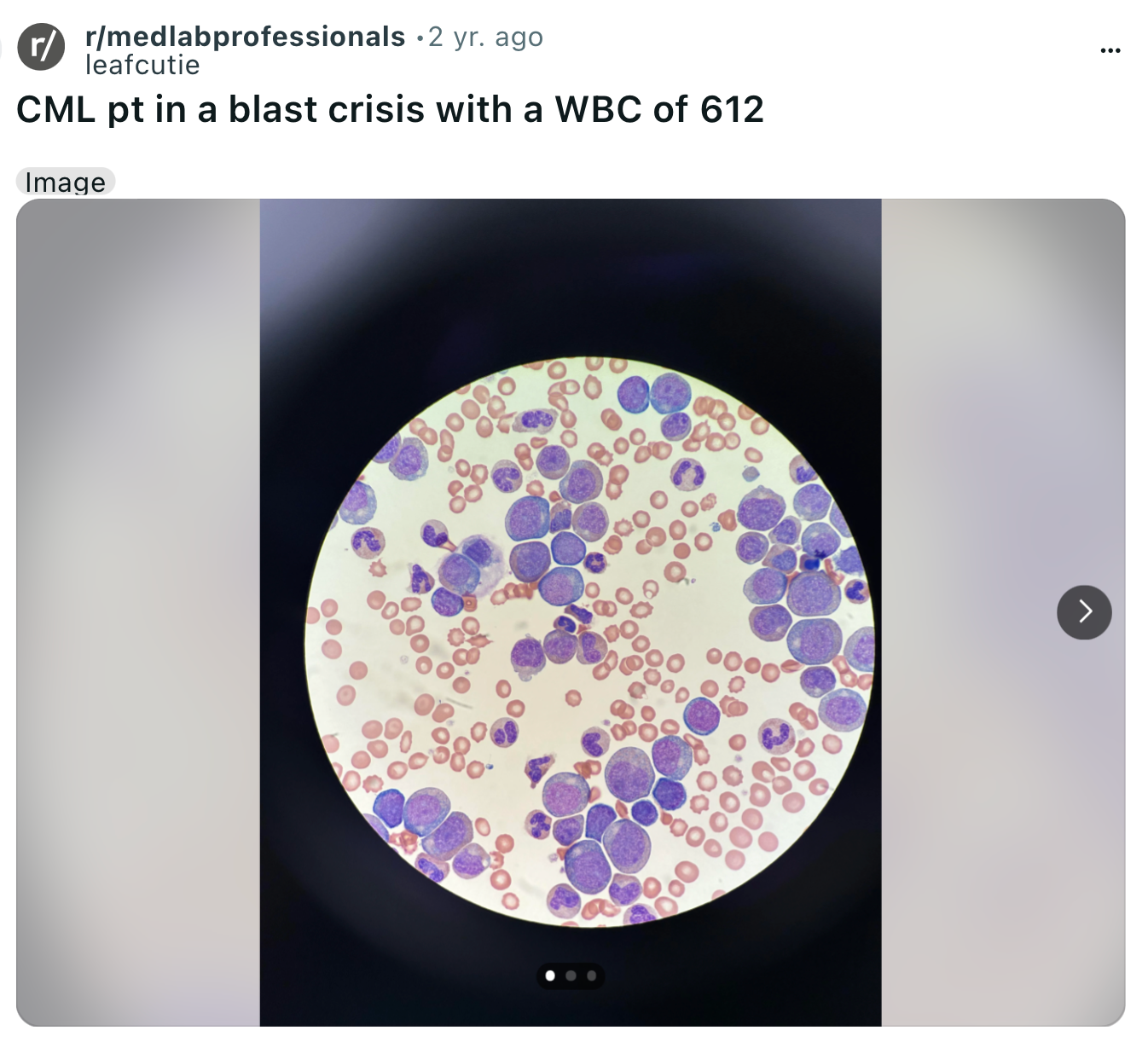
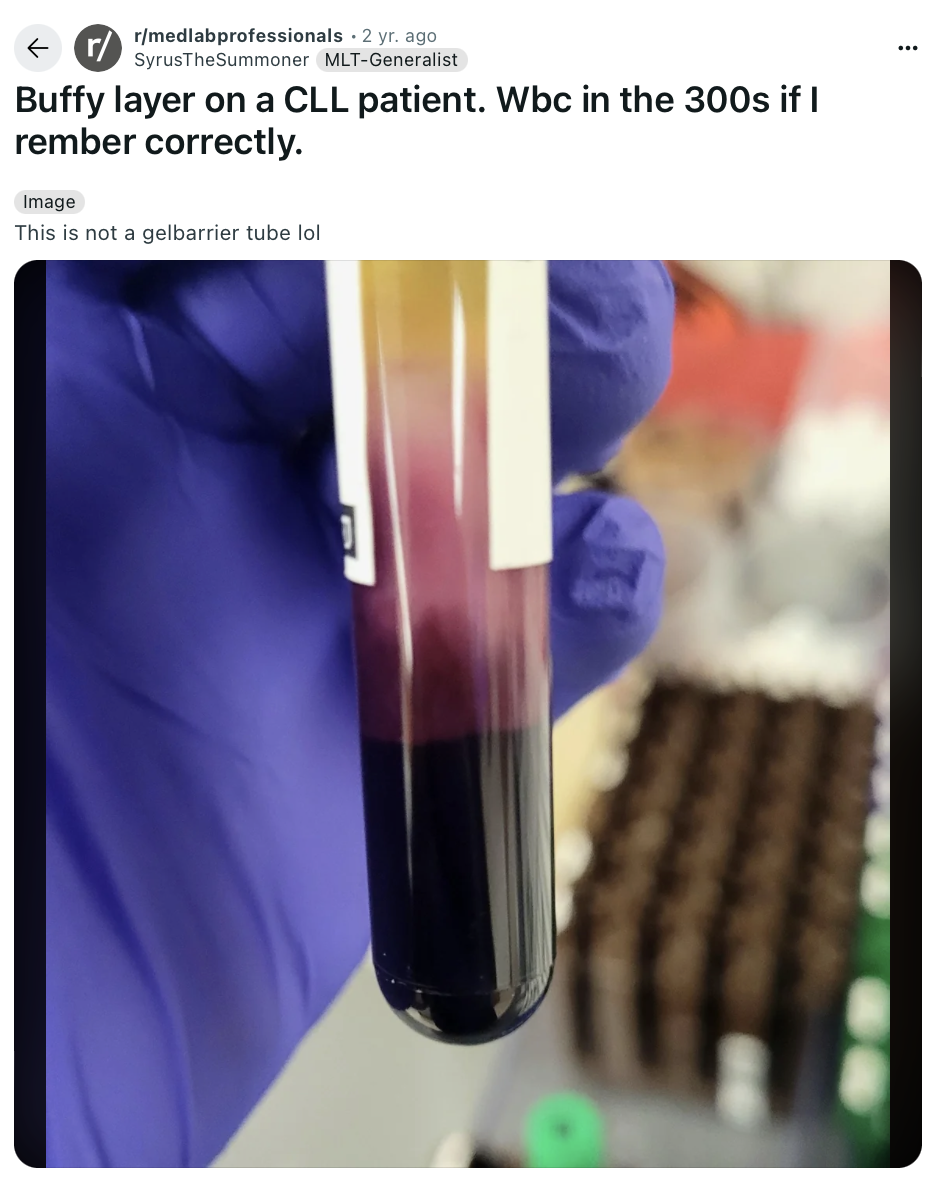
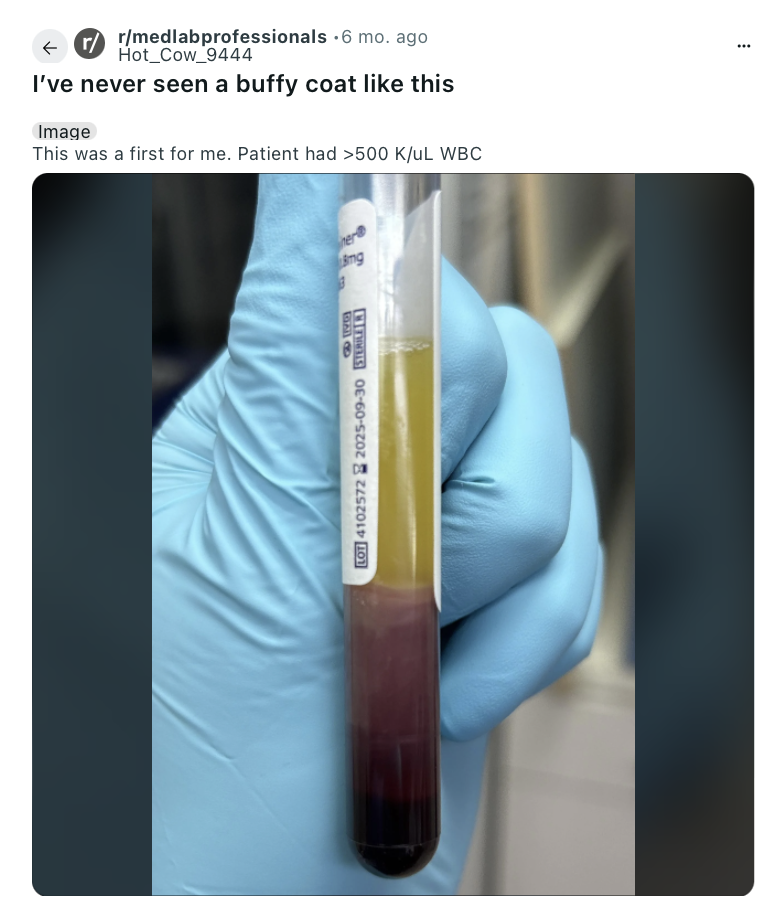
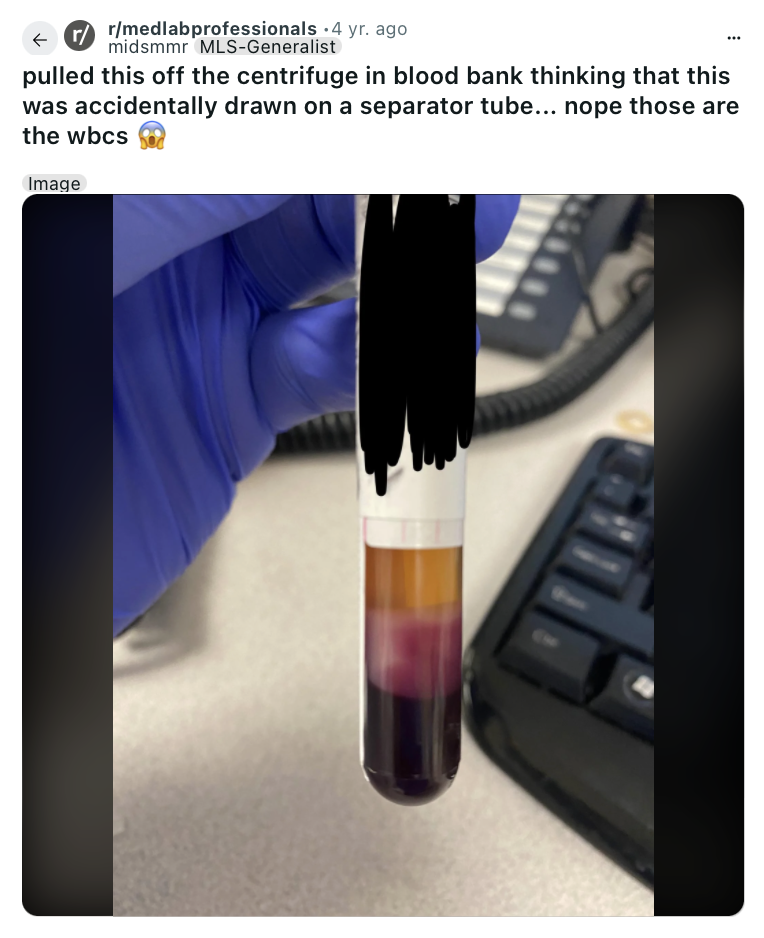
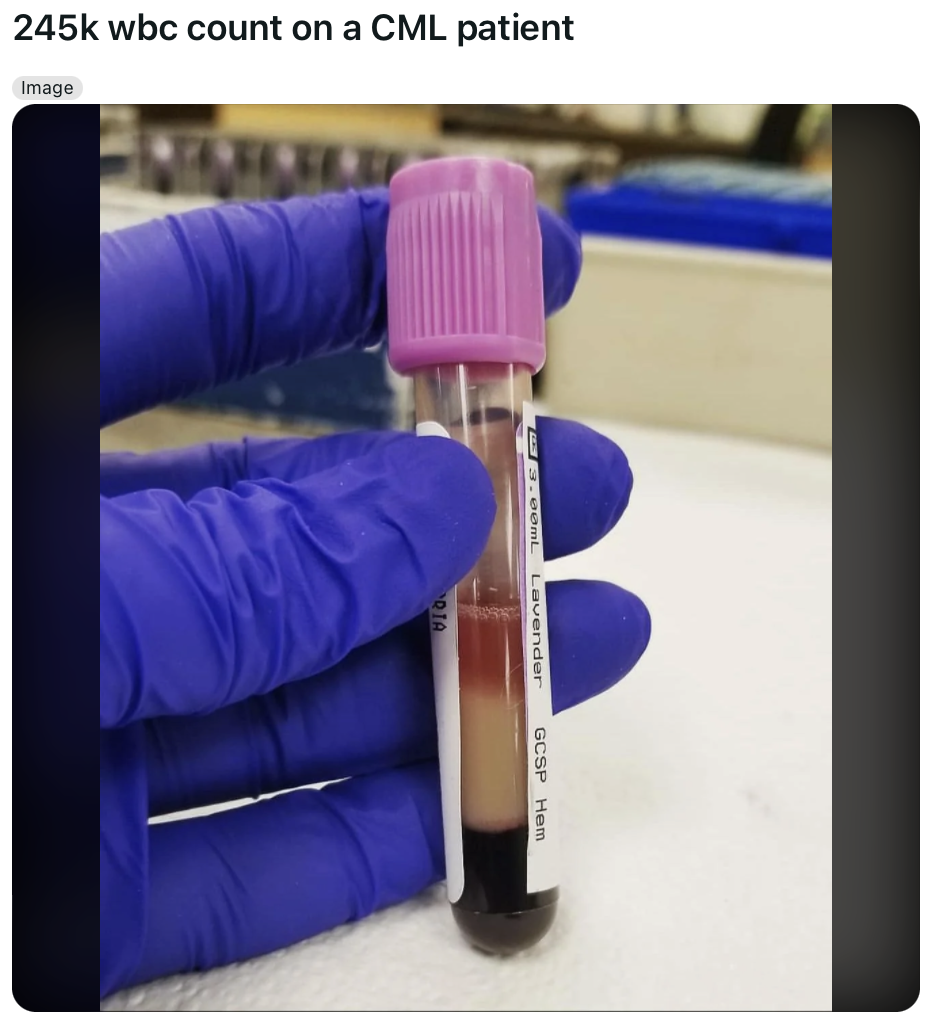
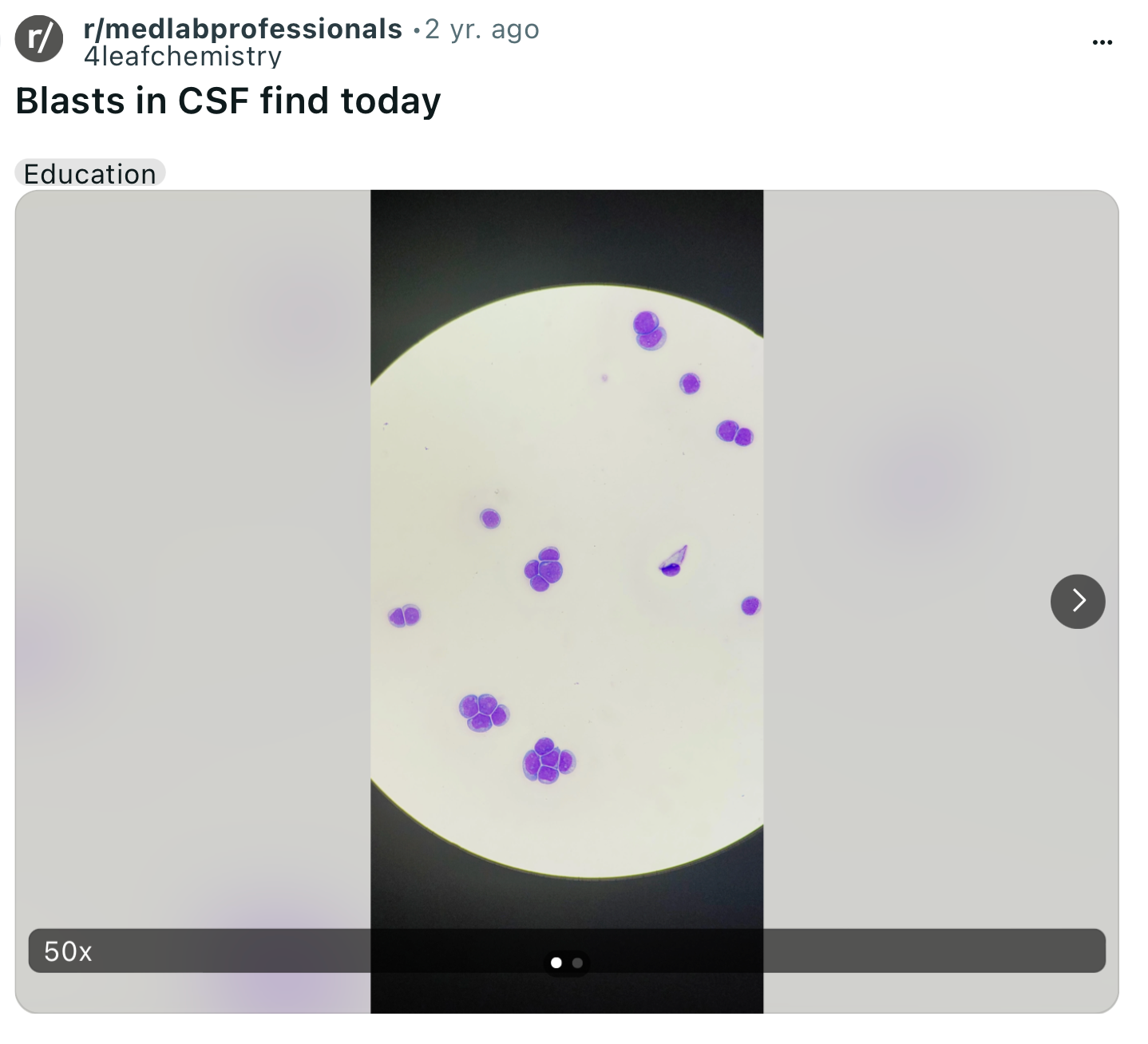
The Leukemia Occurring Right Now Is Next Level... Like Beyond What Experienced Lab Techs Have Ever Seen
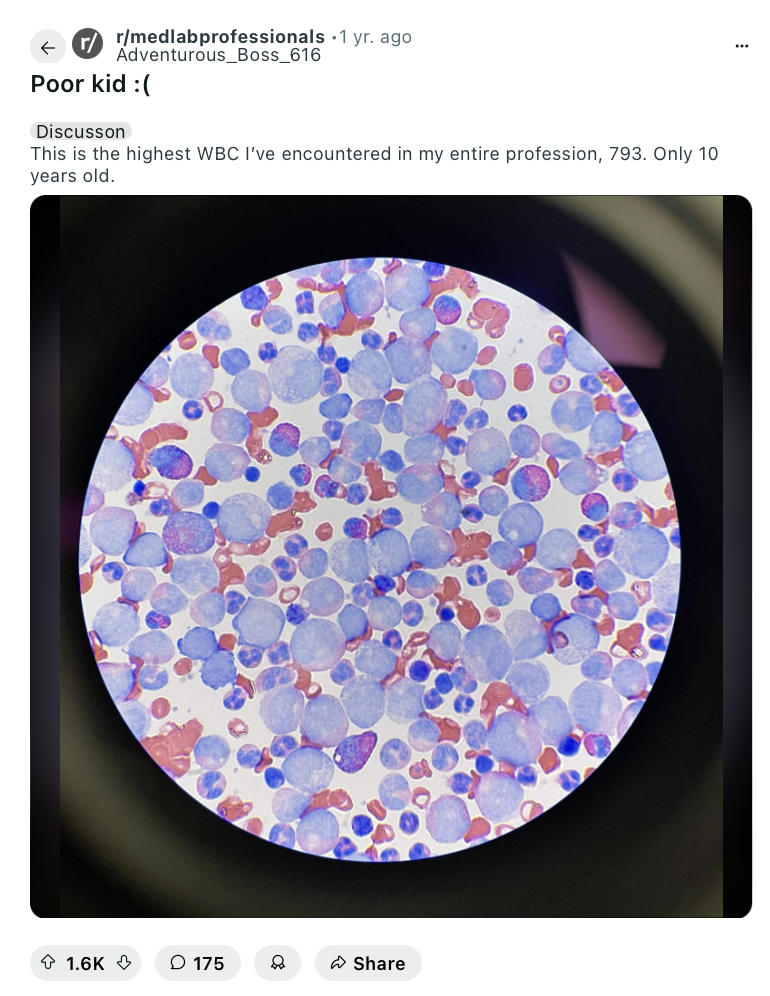
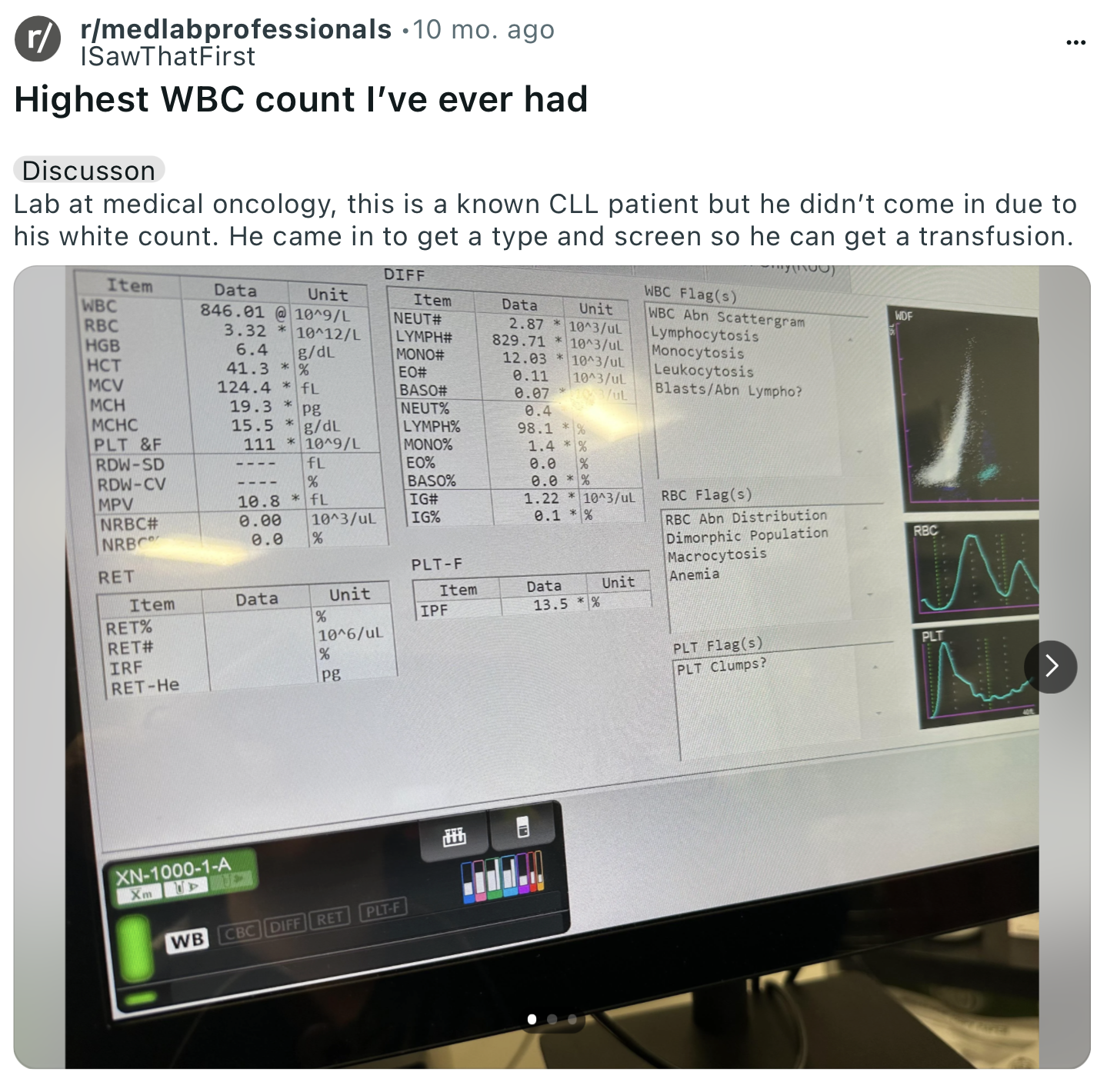
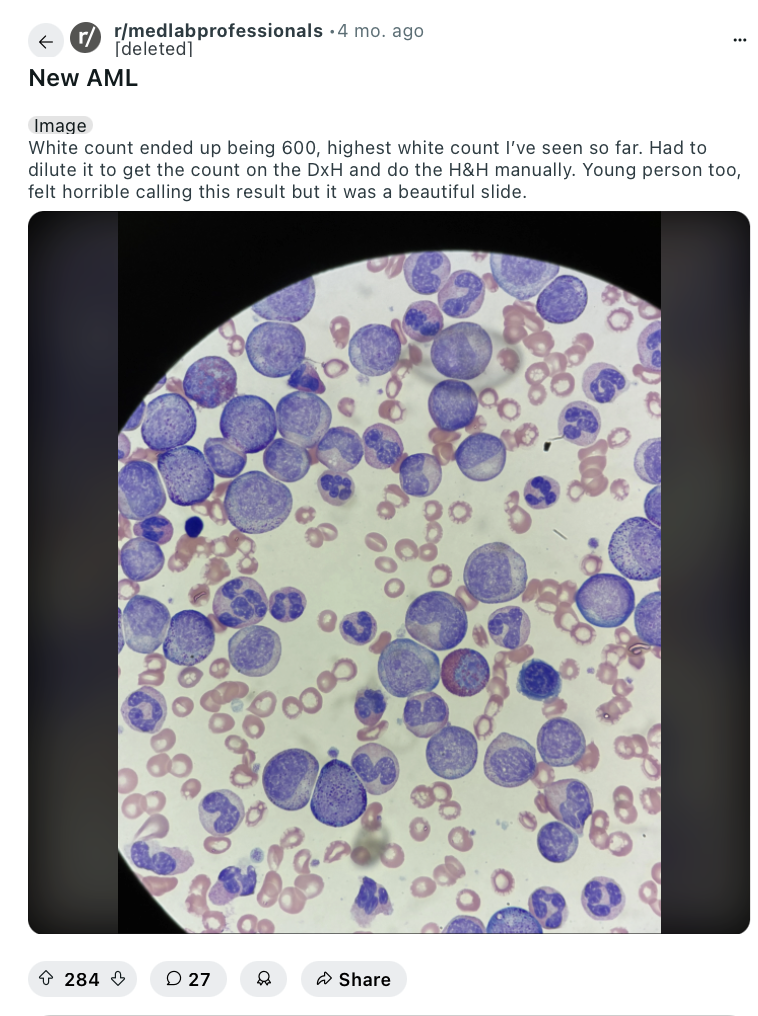
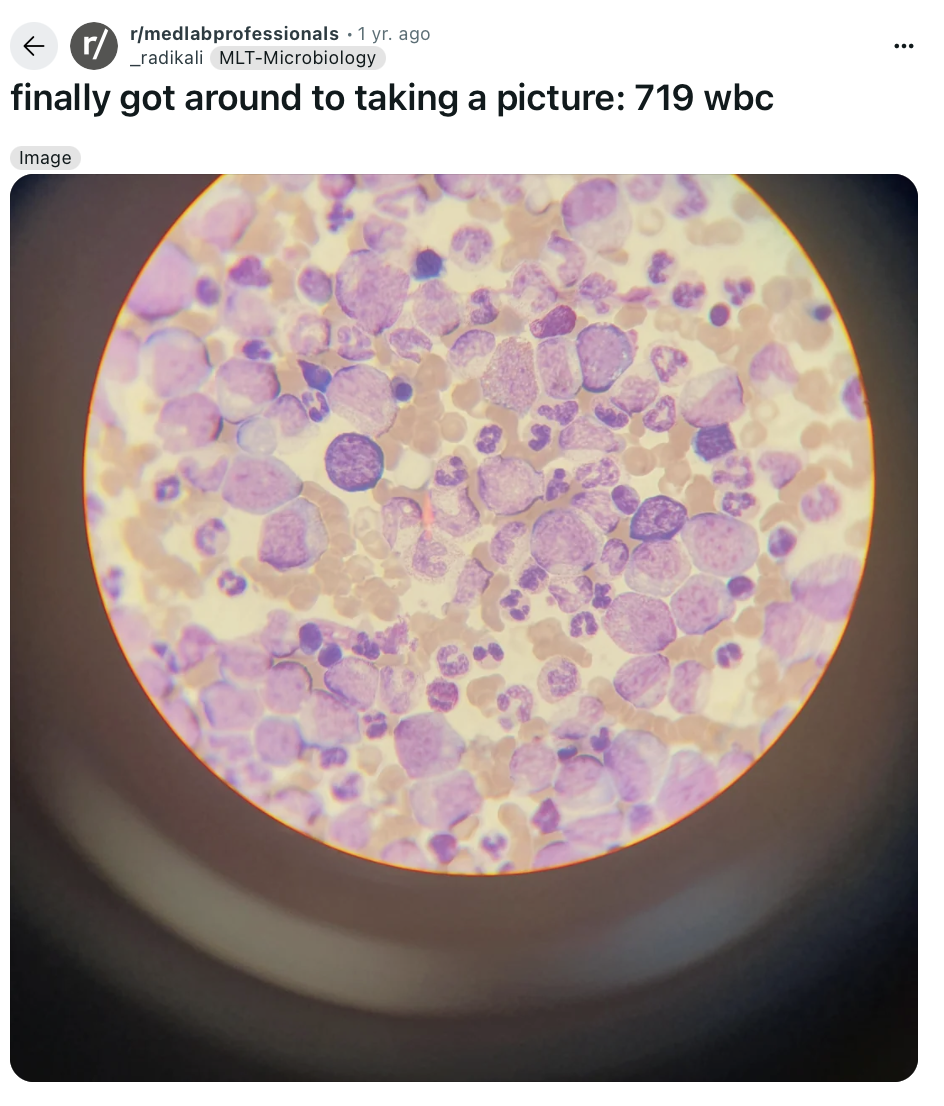
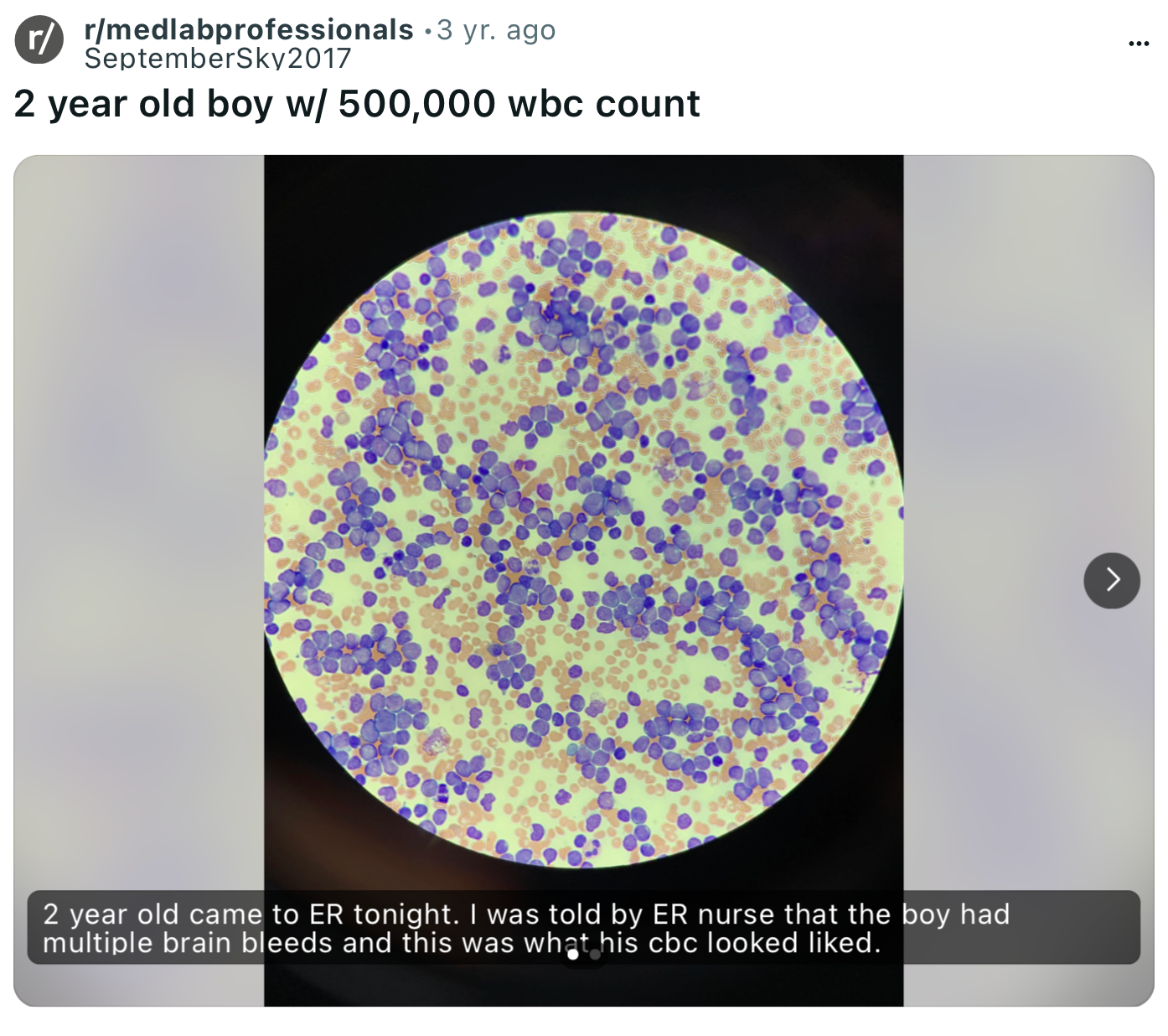
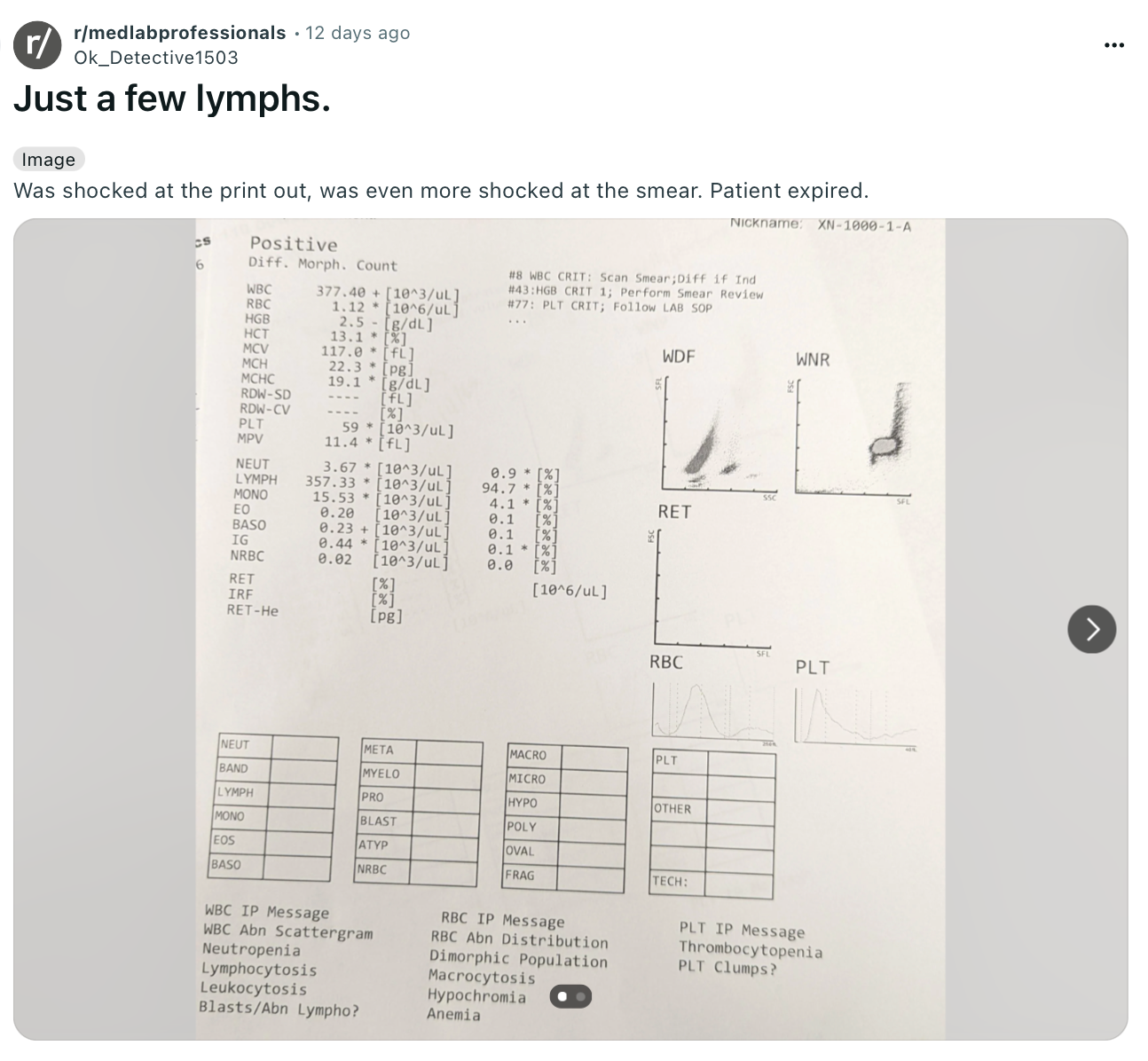
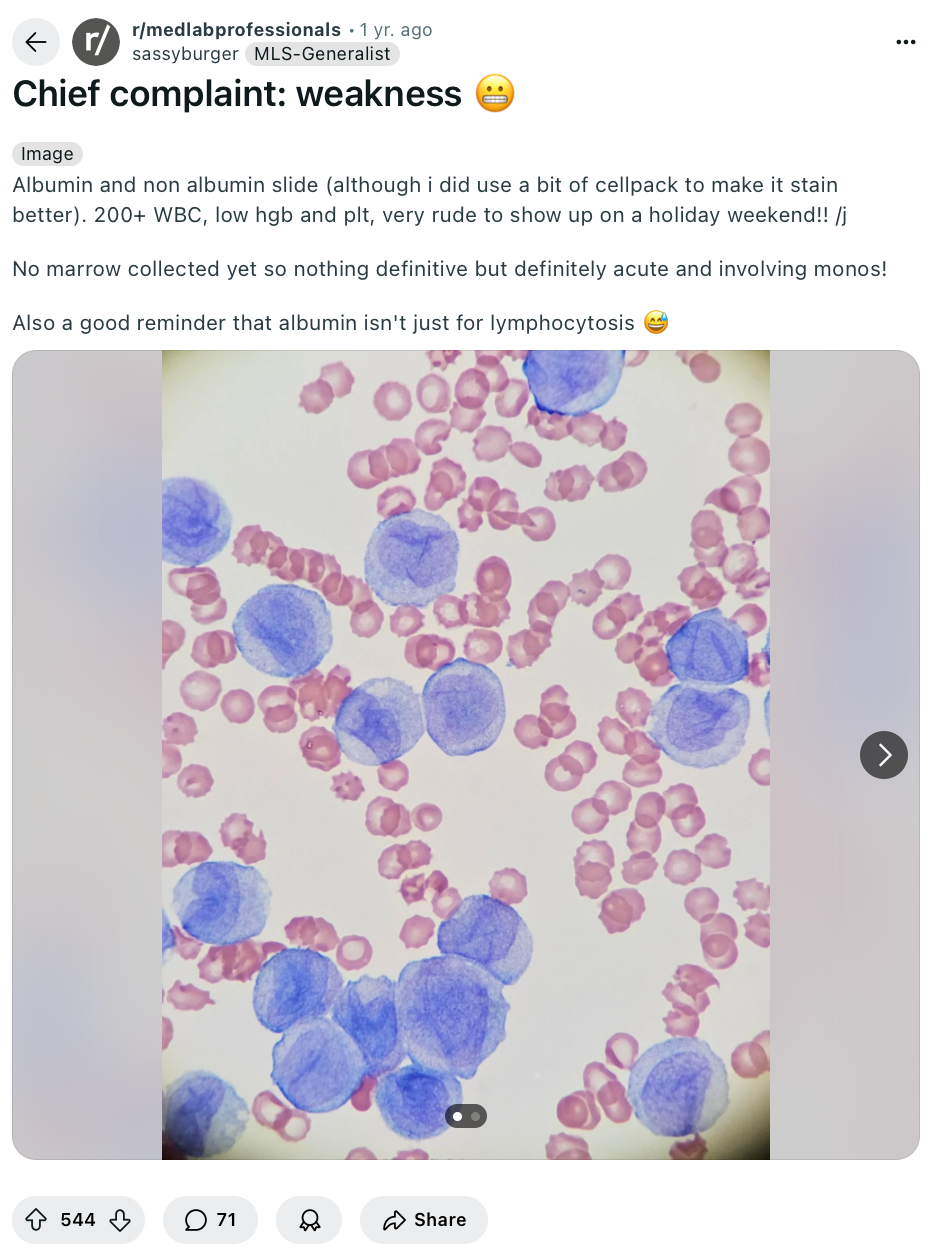
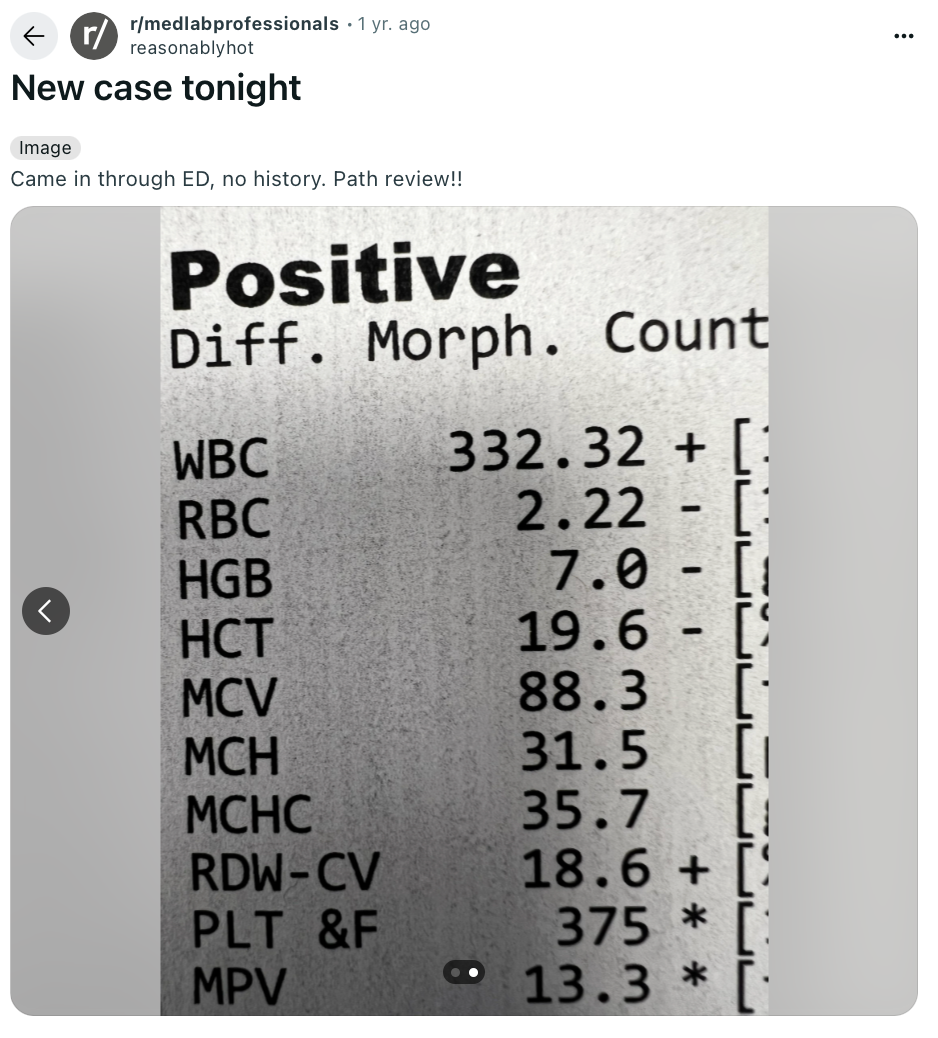
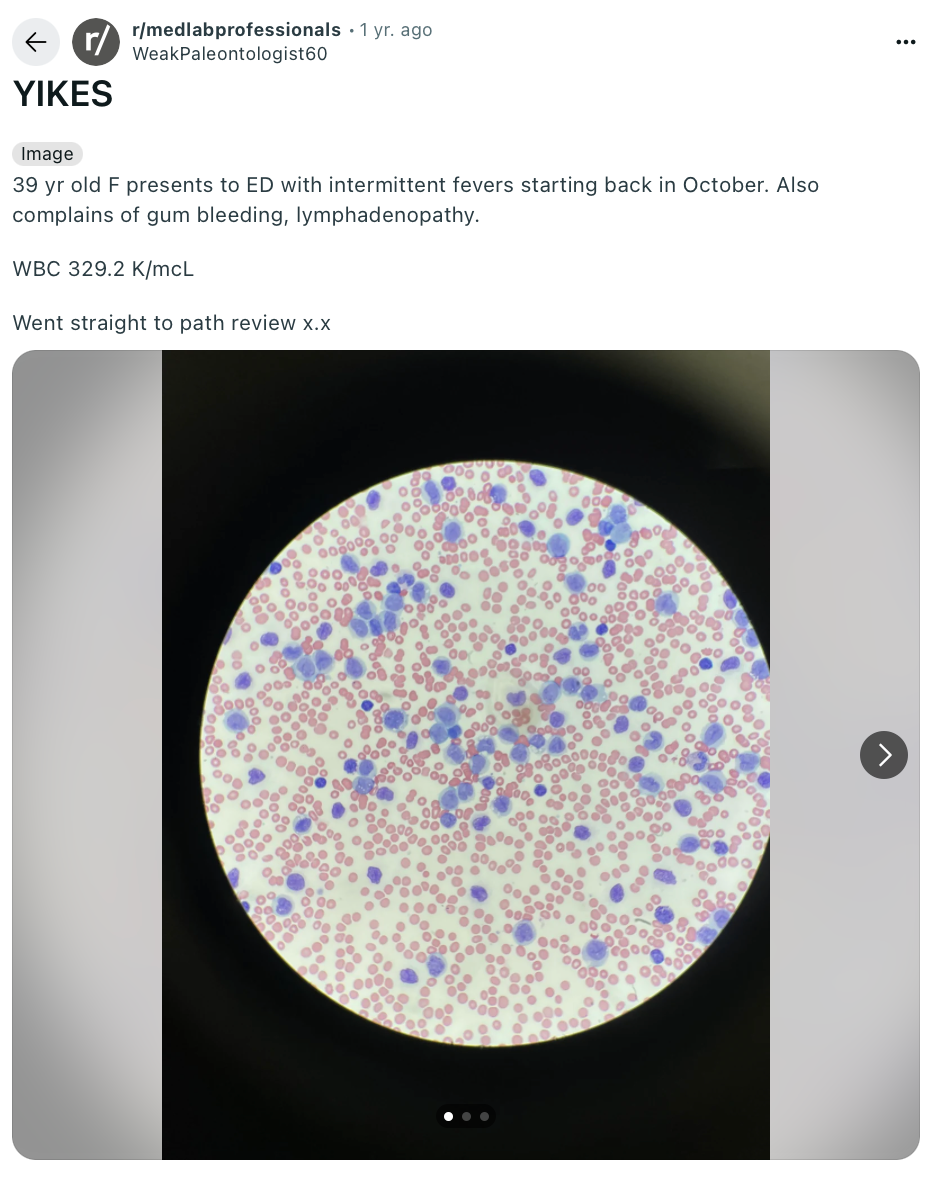
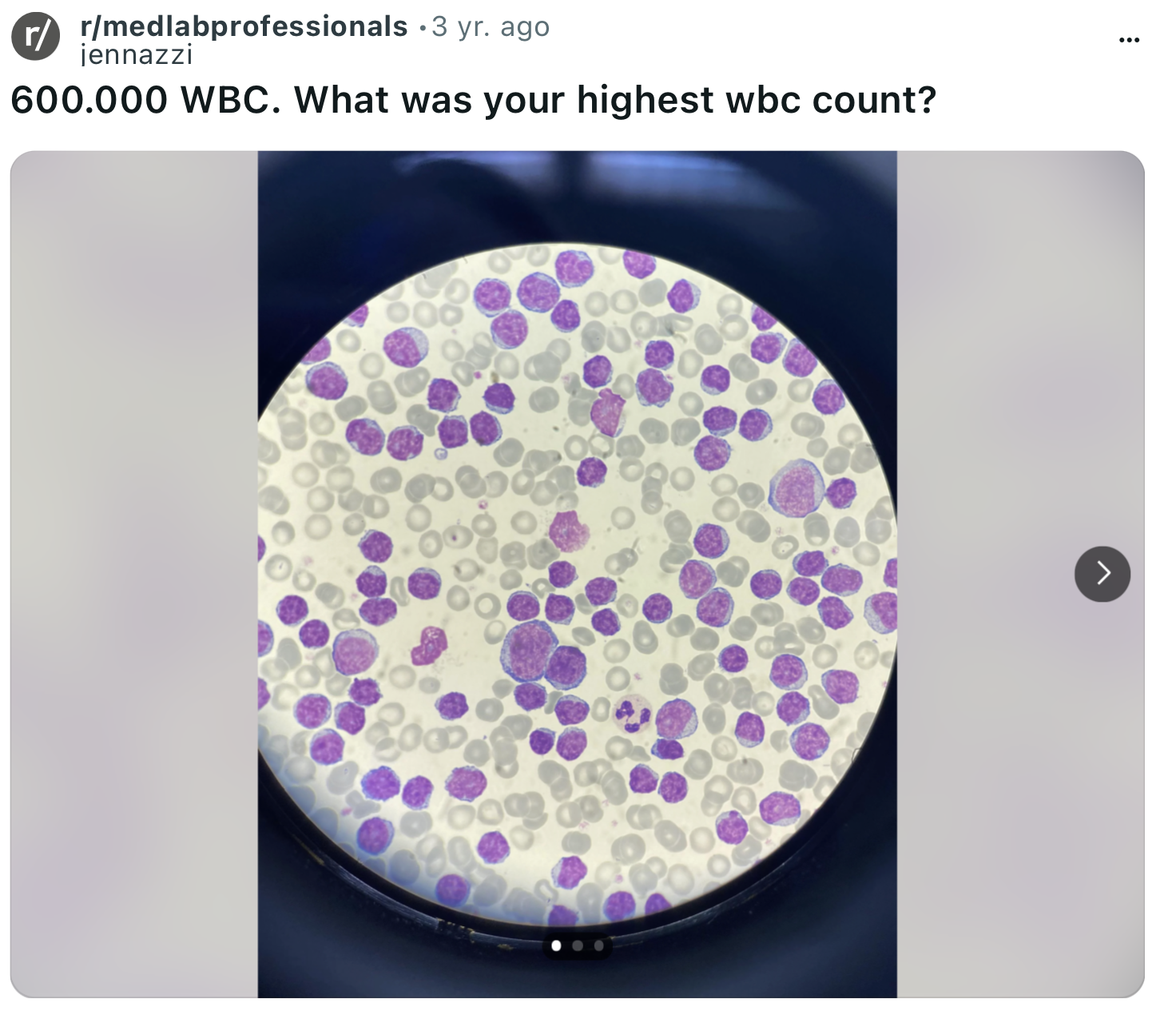
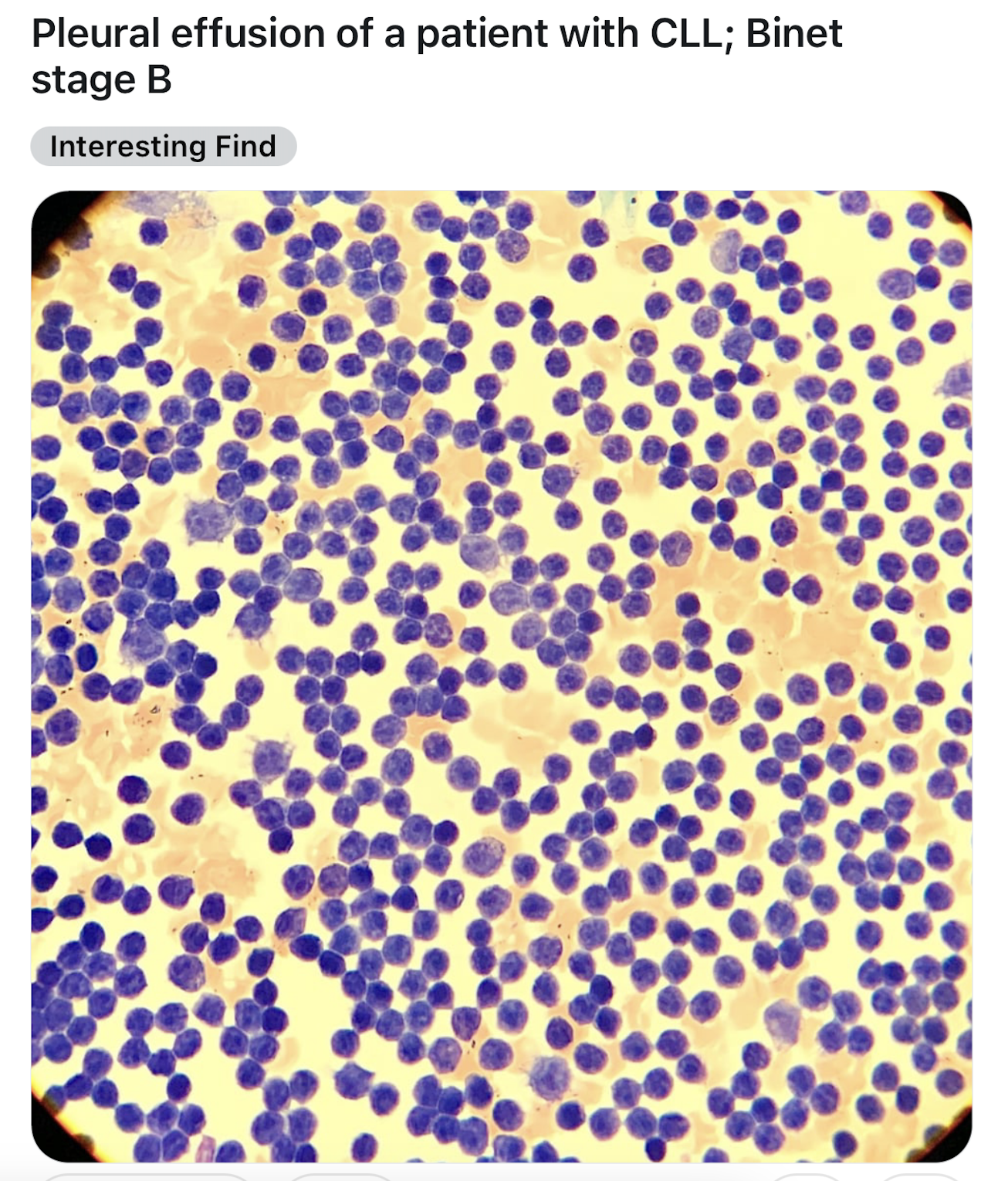
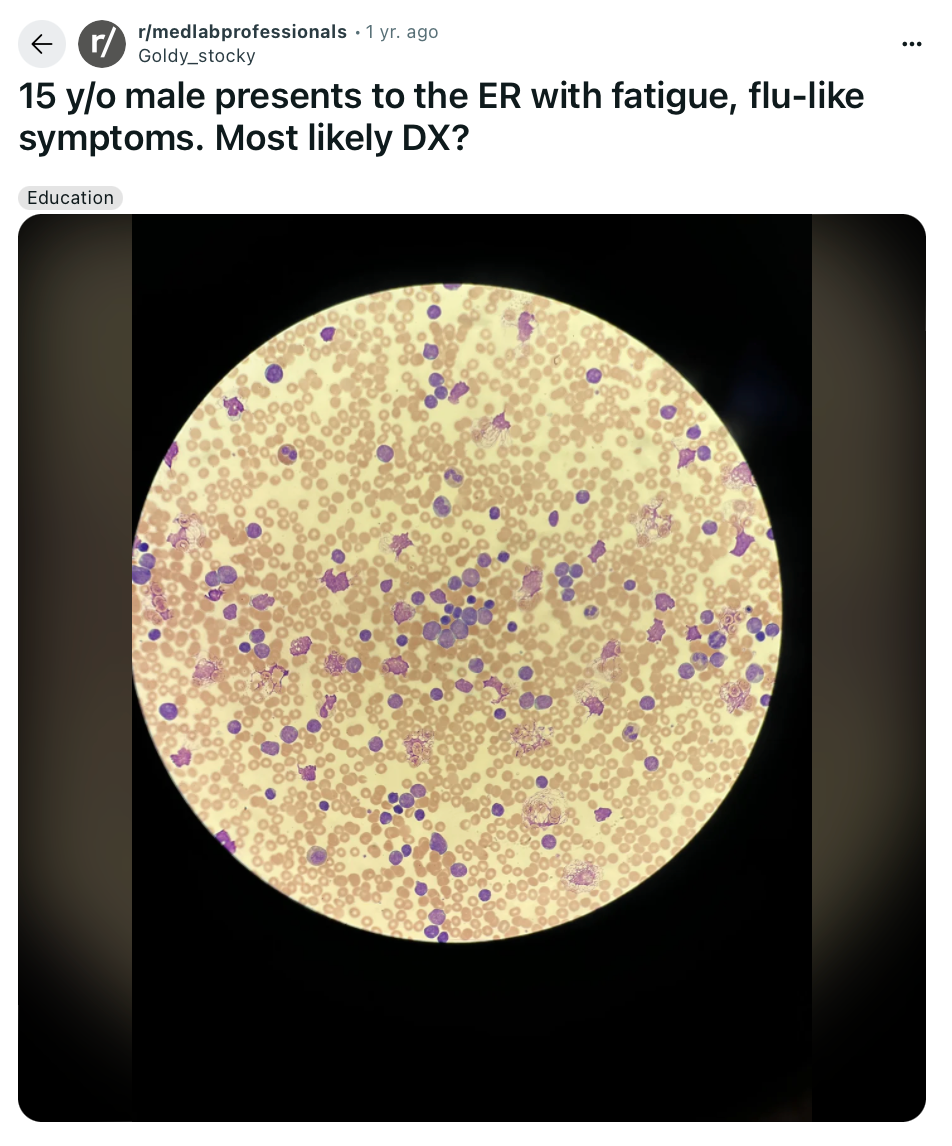
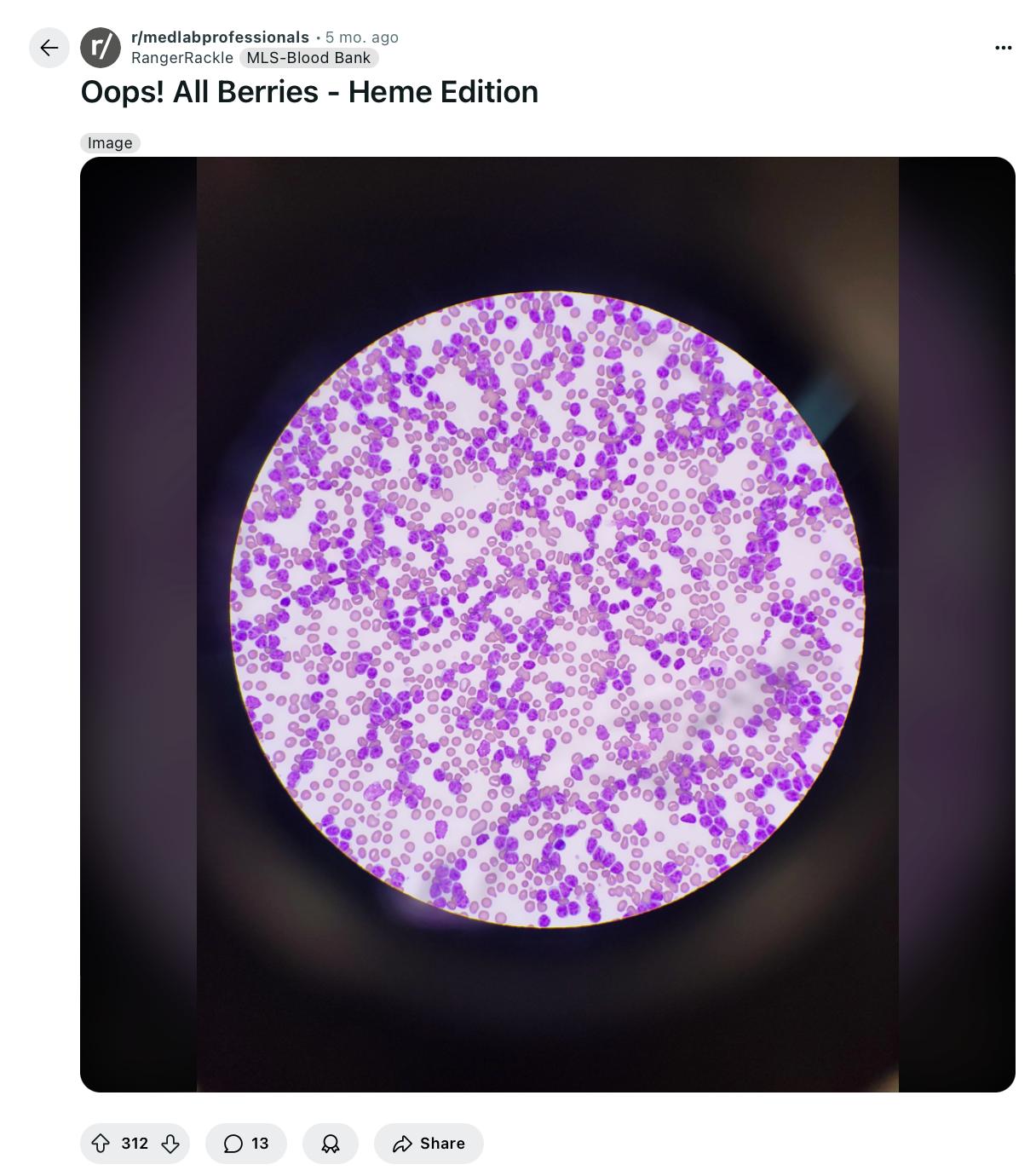
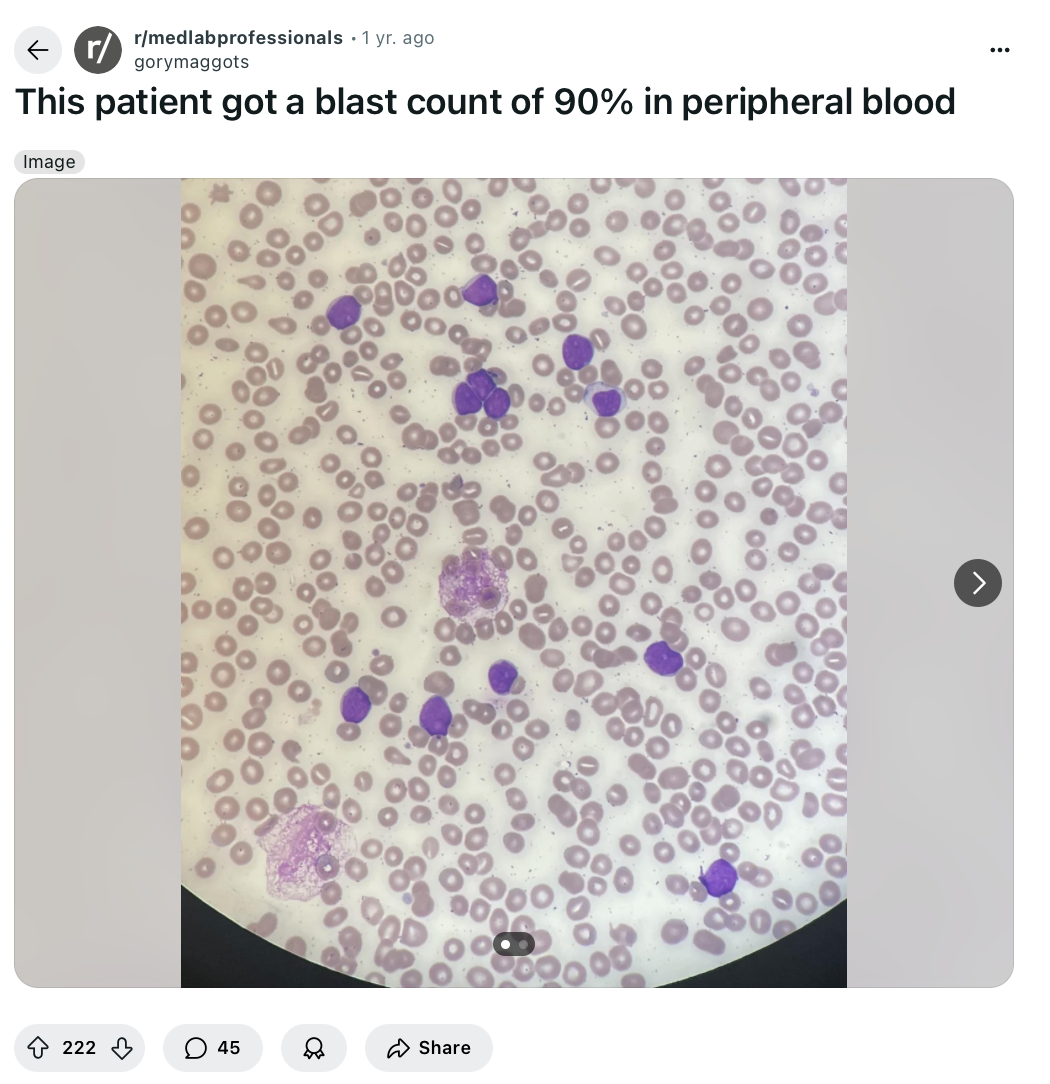
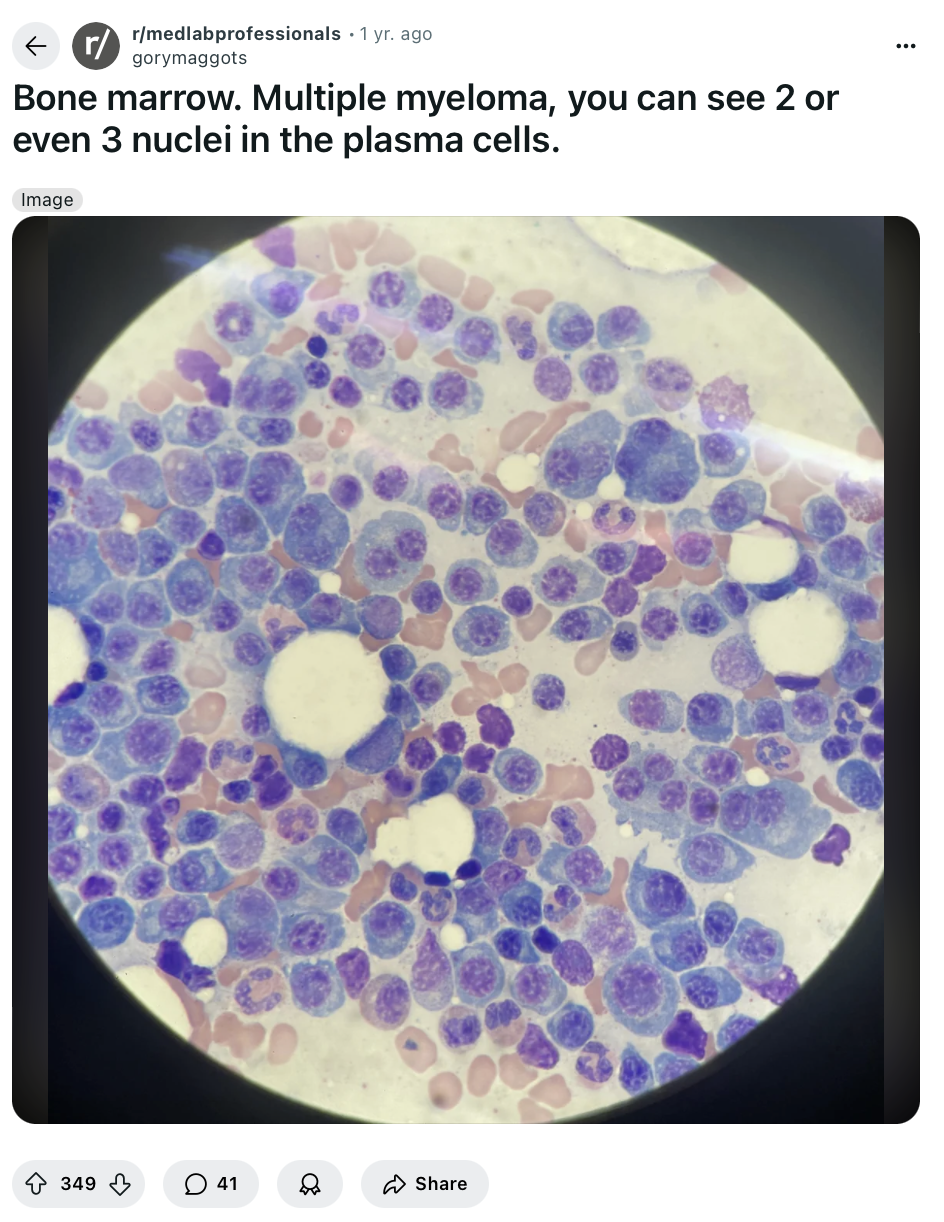
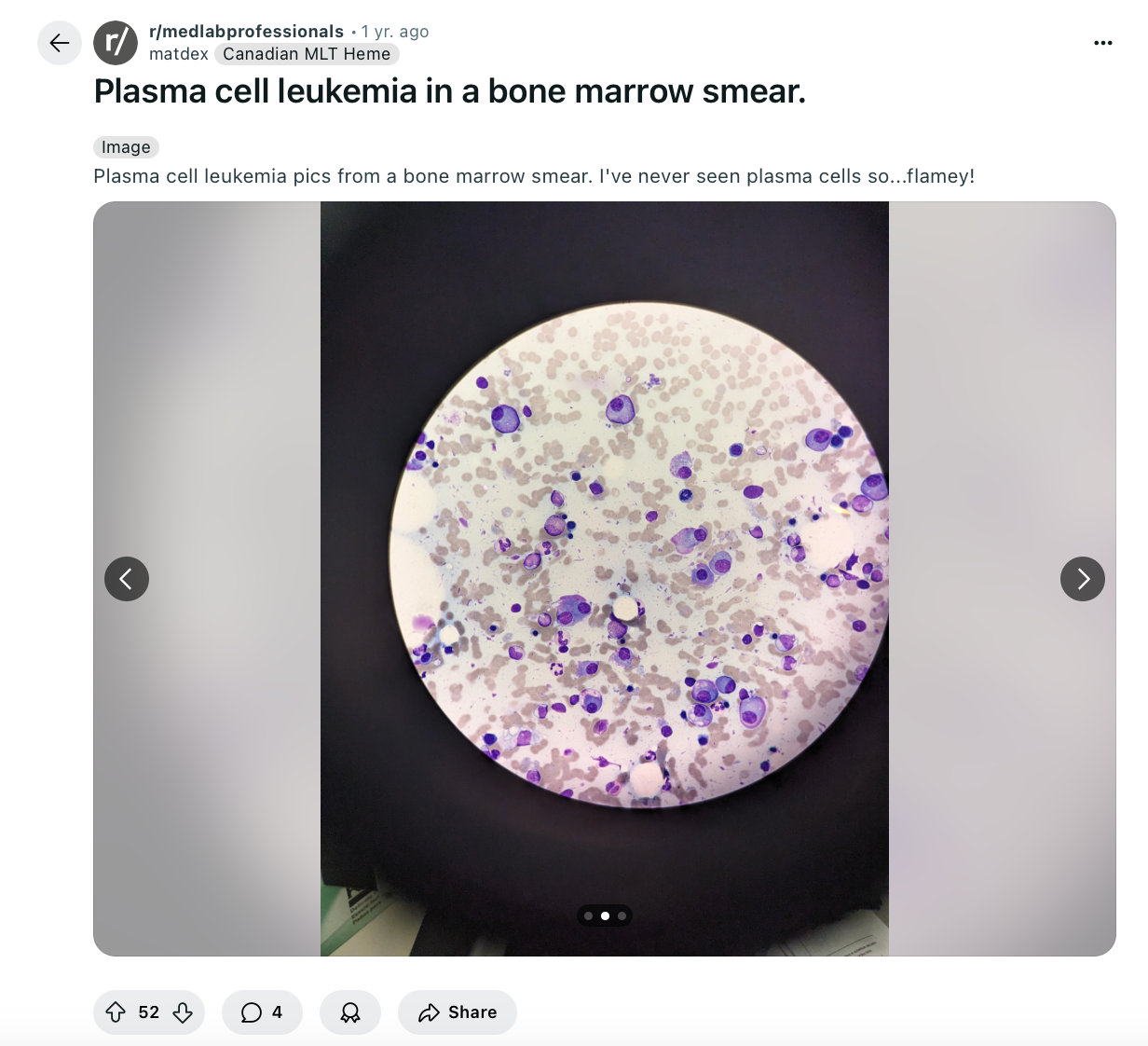
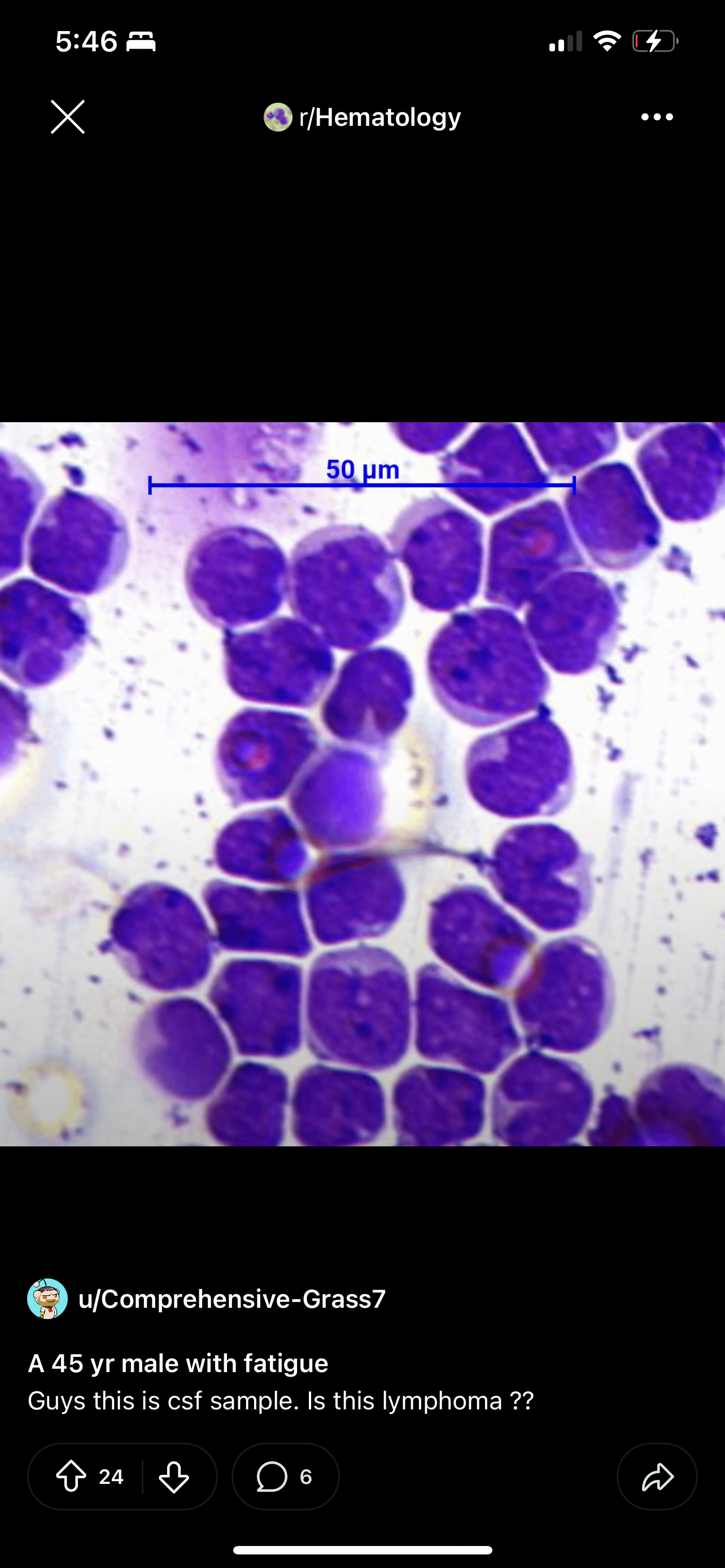
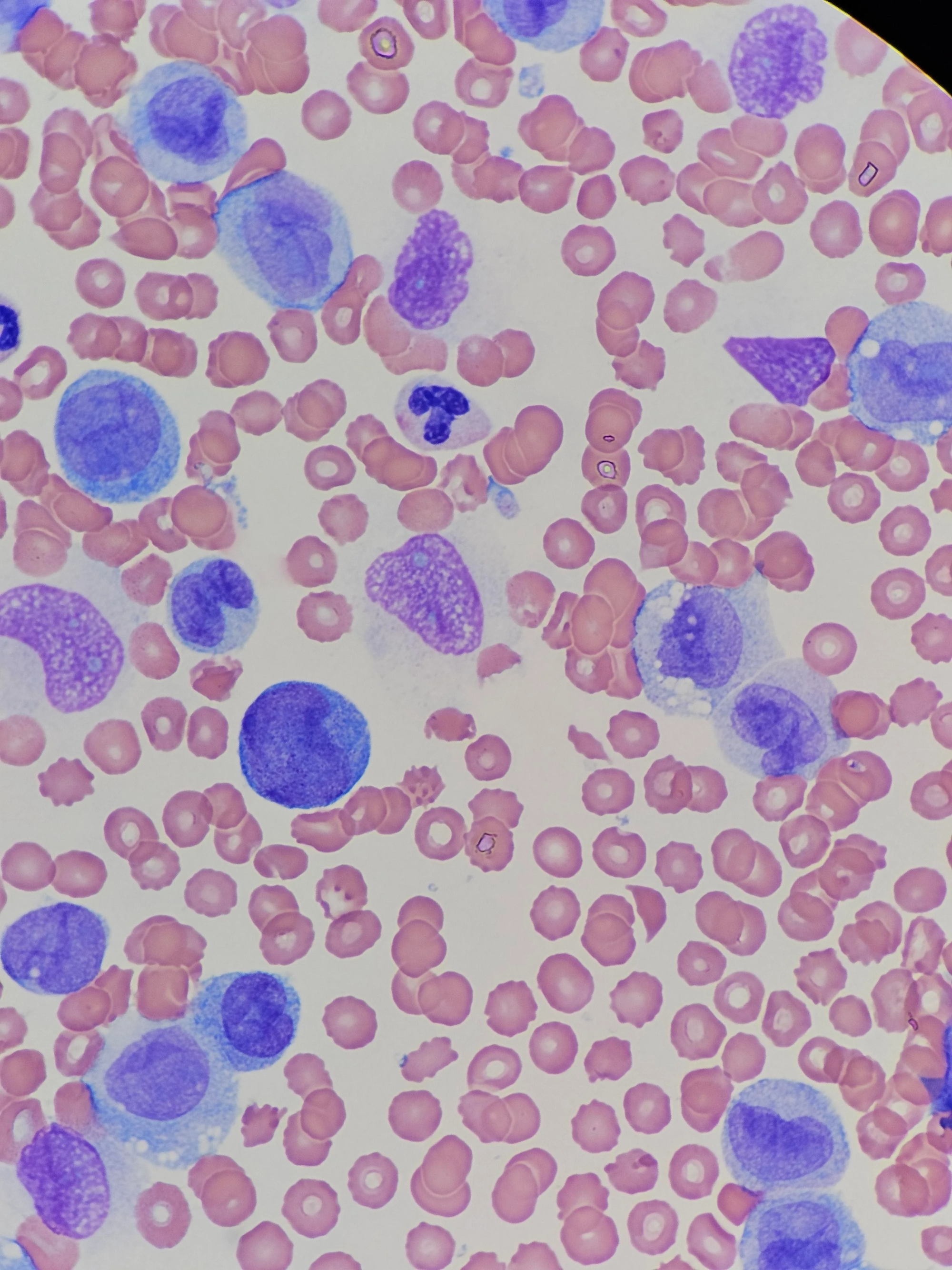
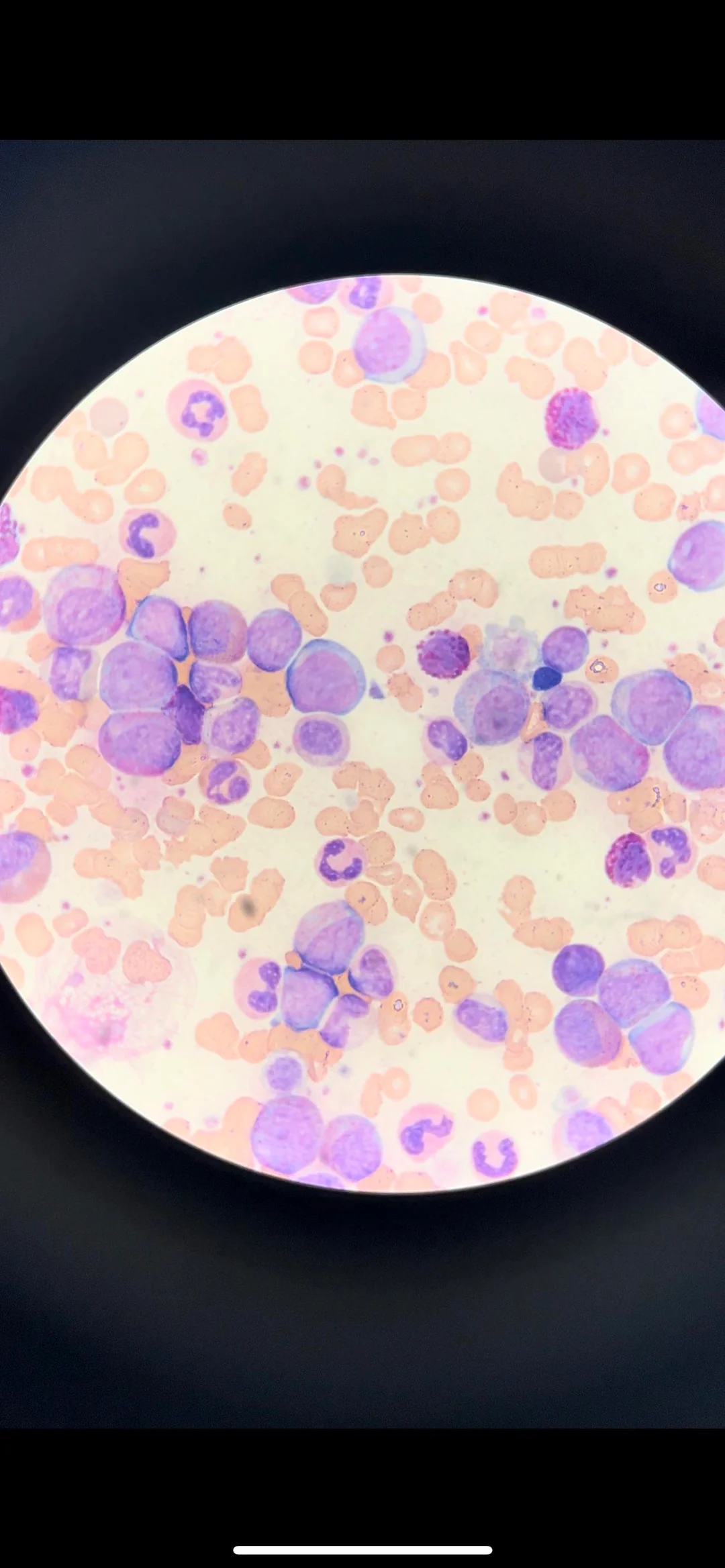
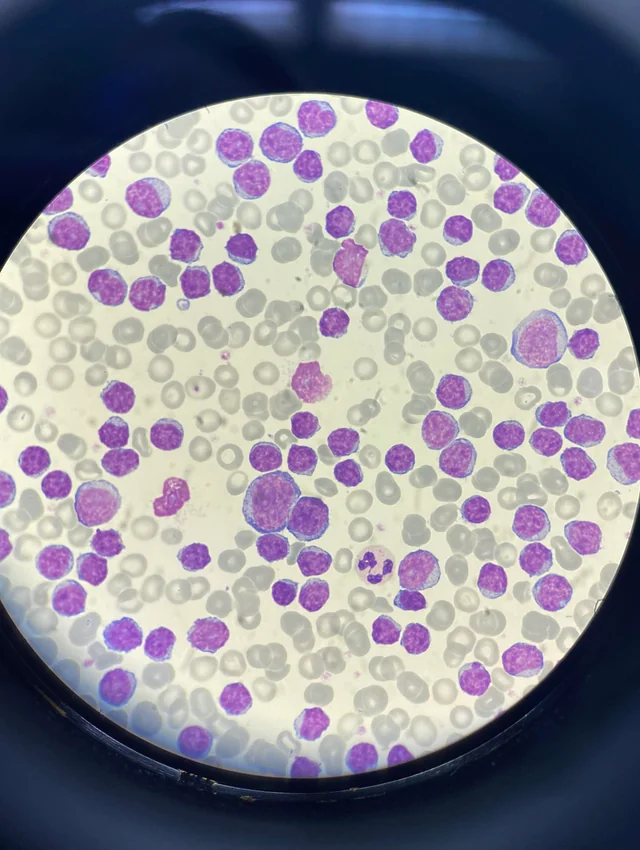
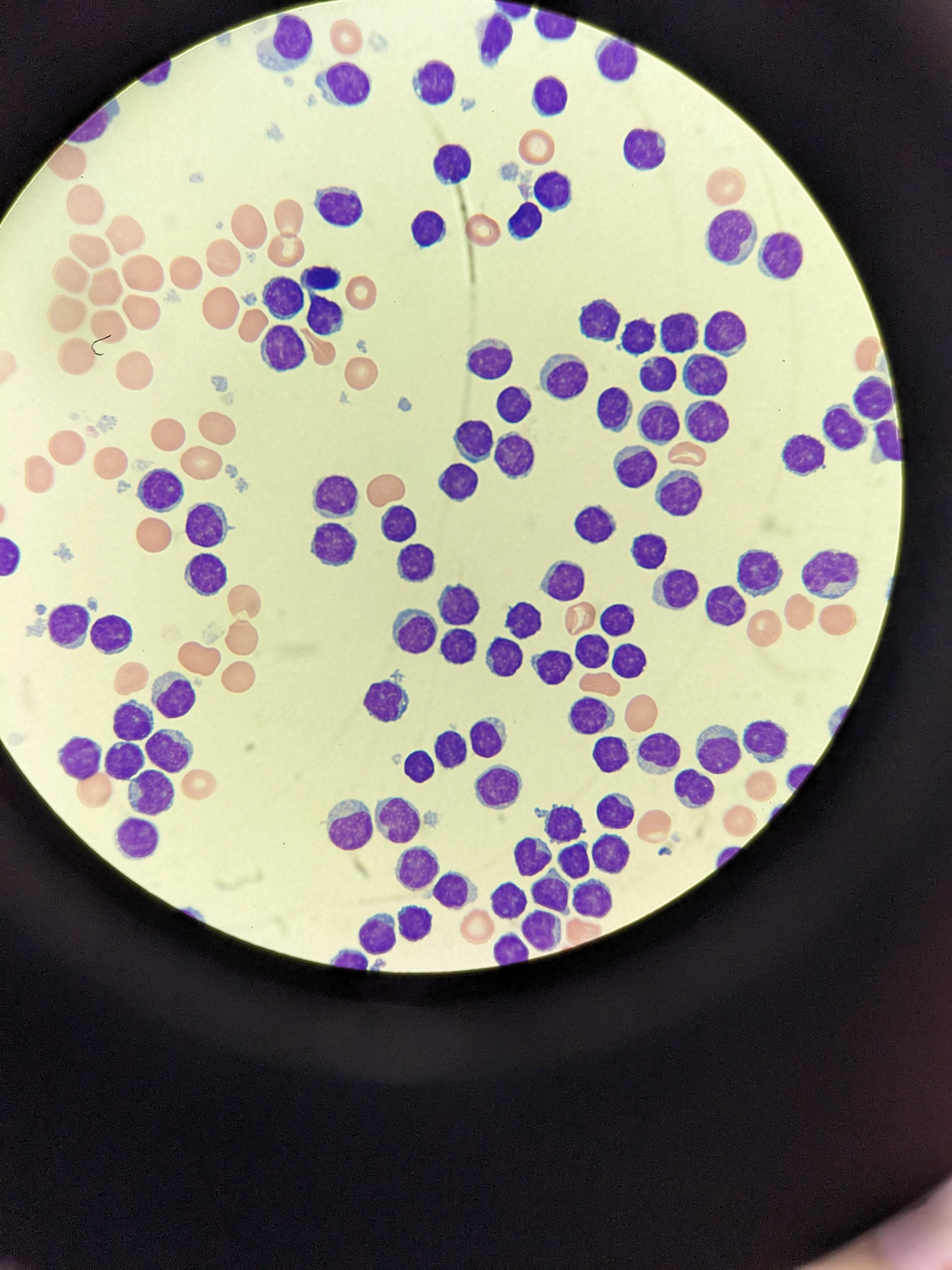
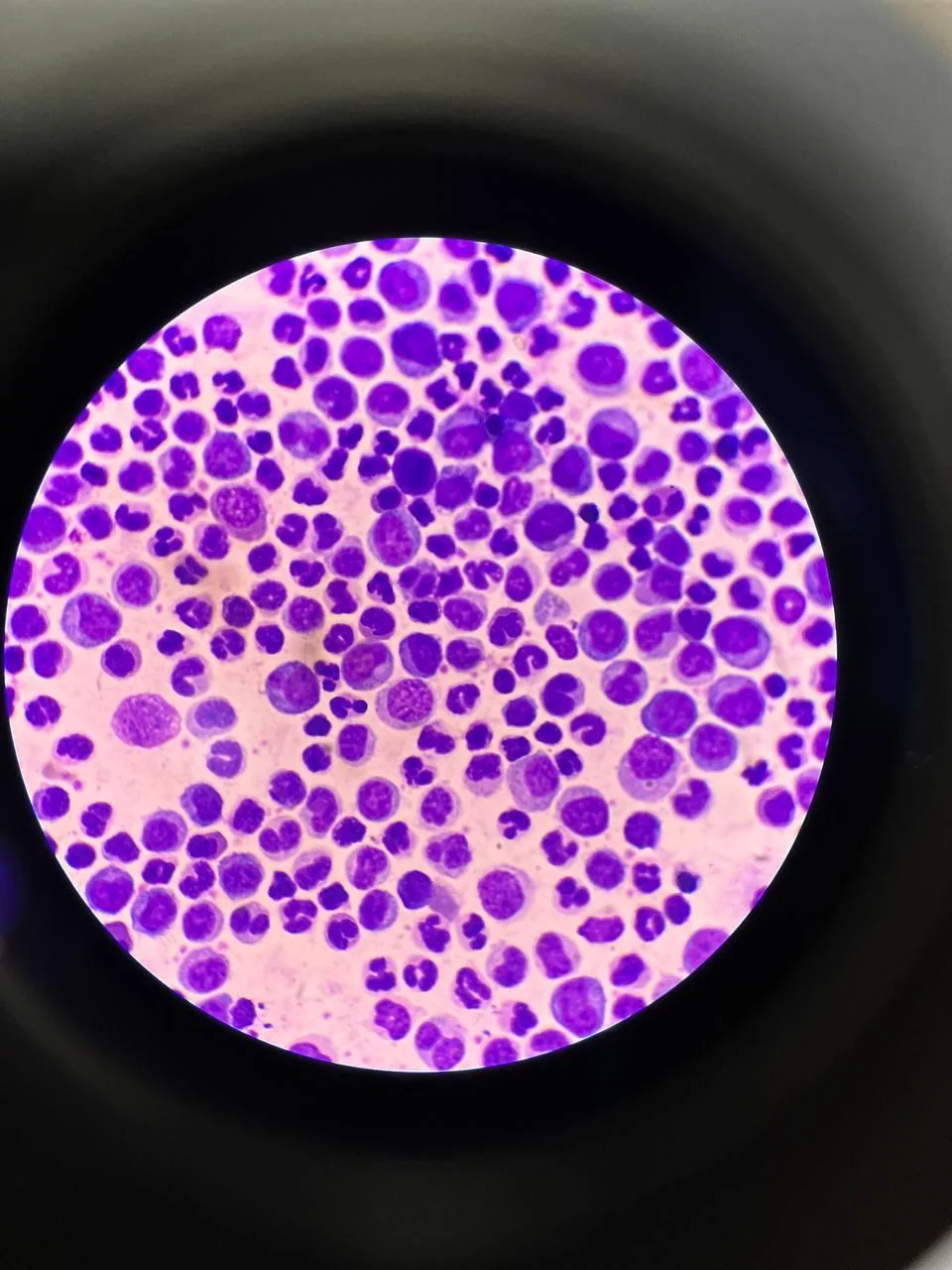
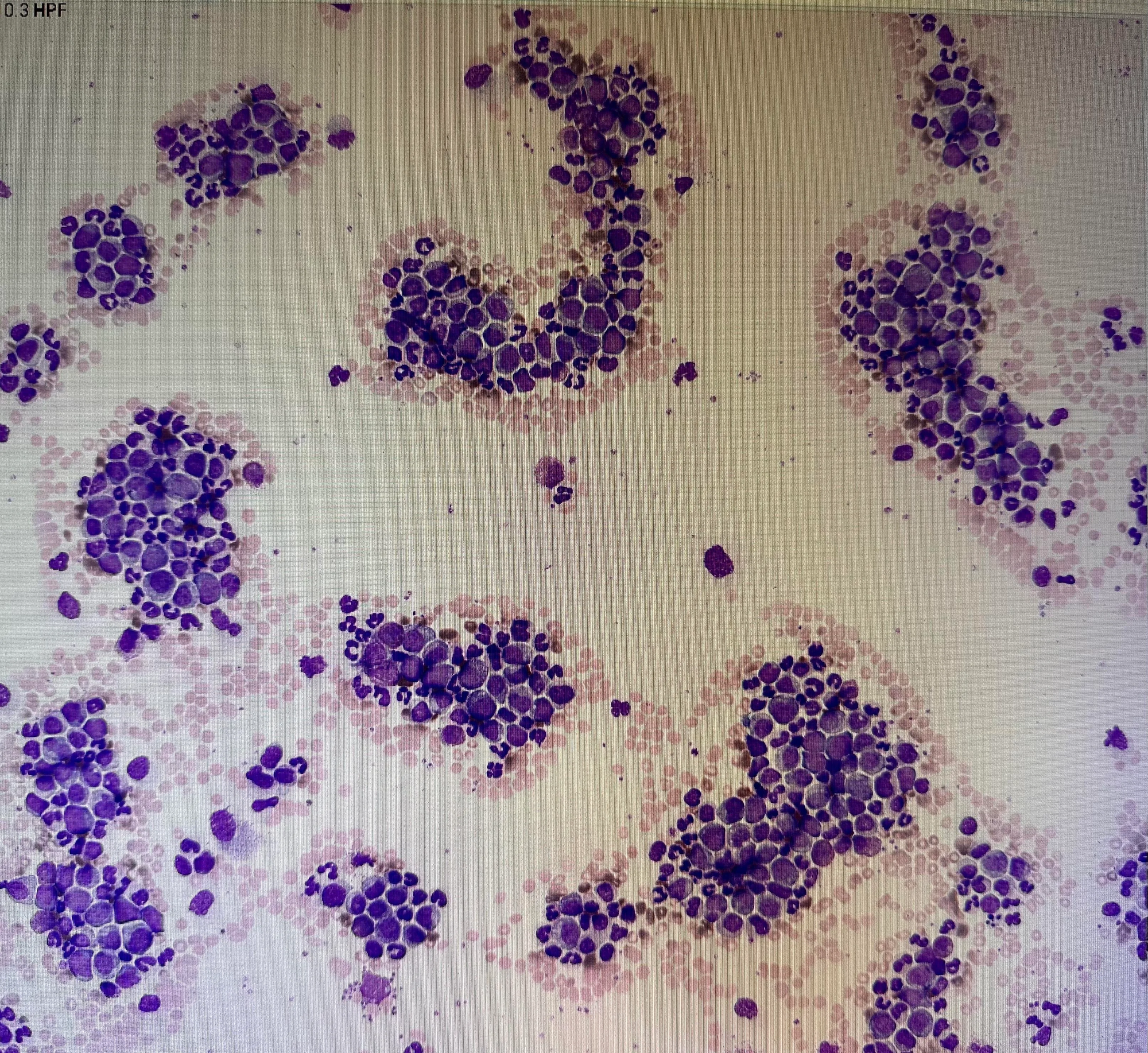
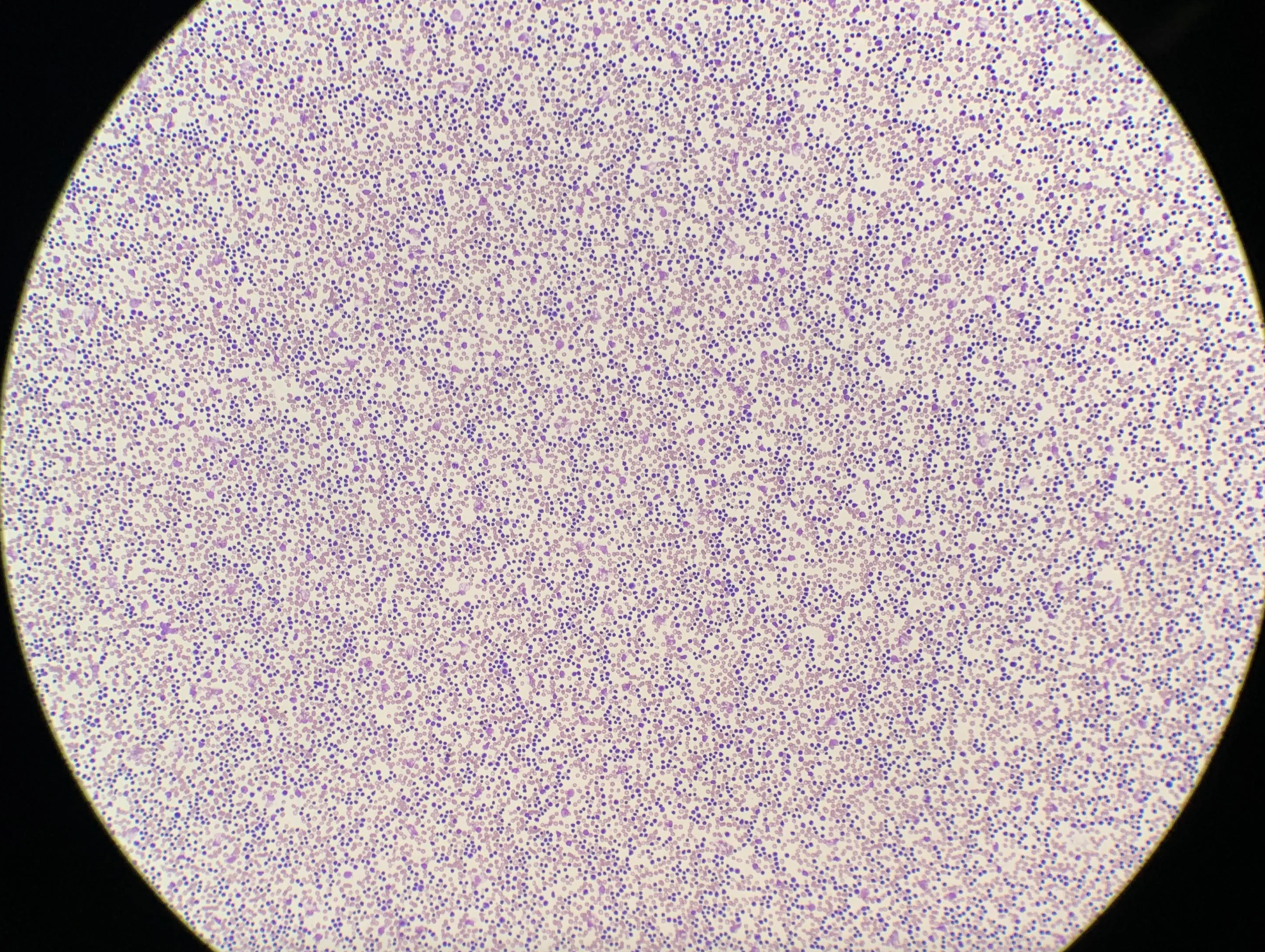
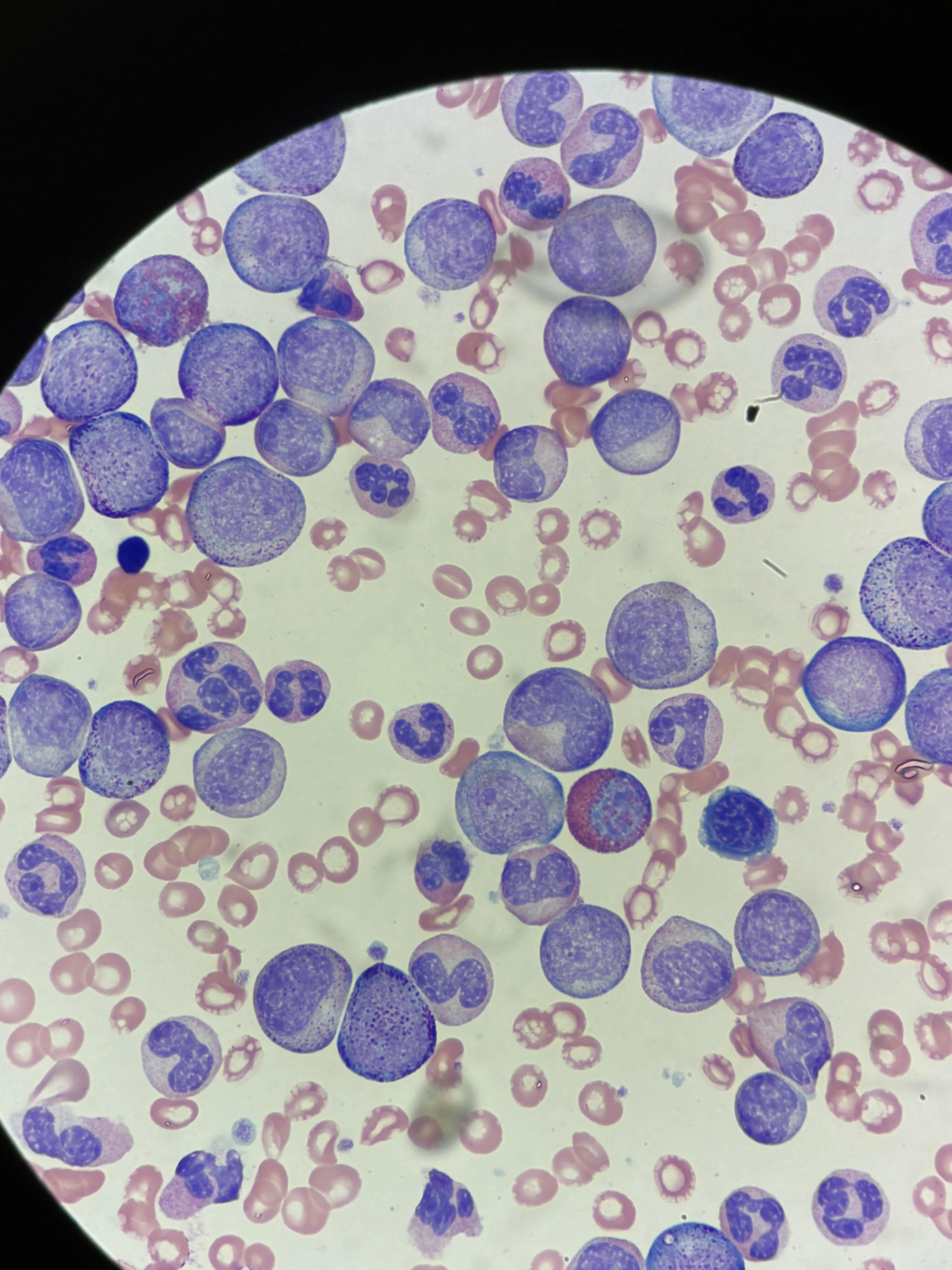
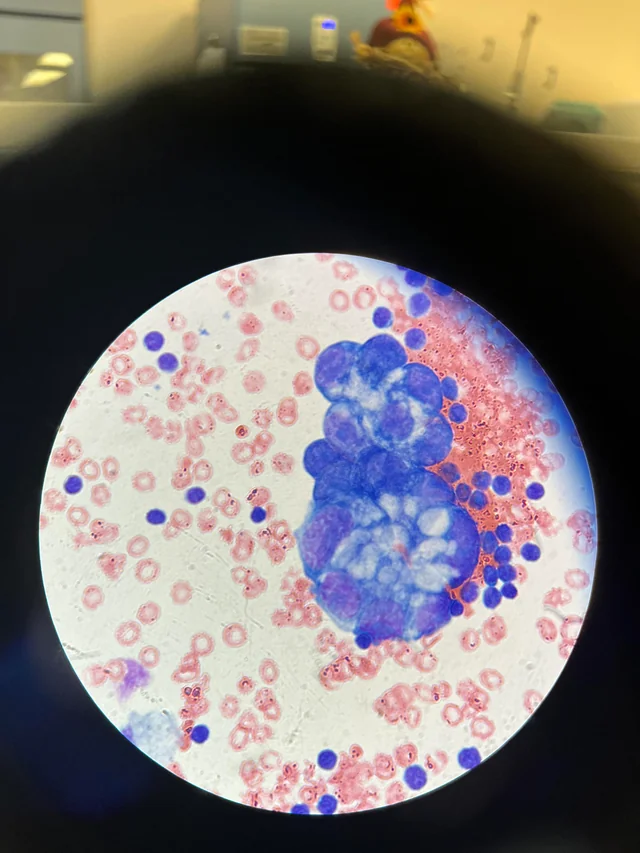
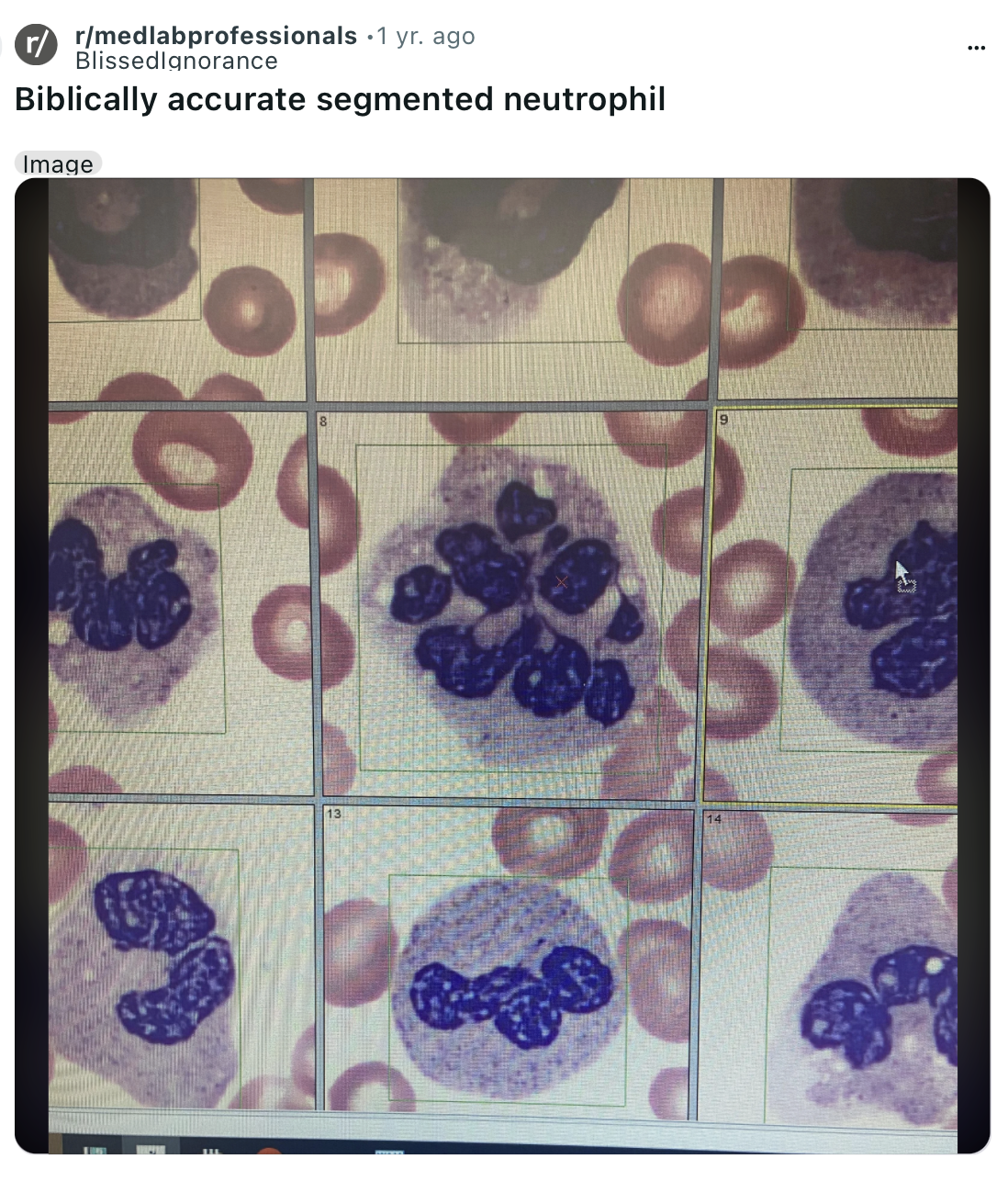
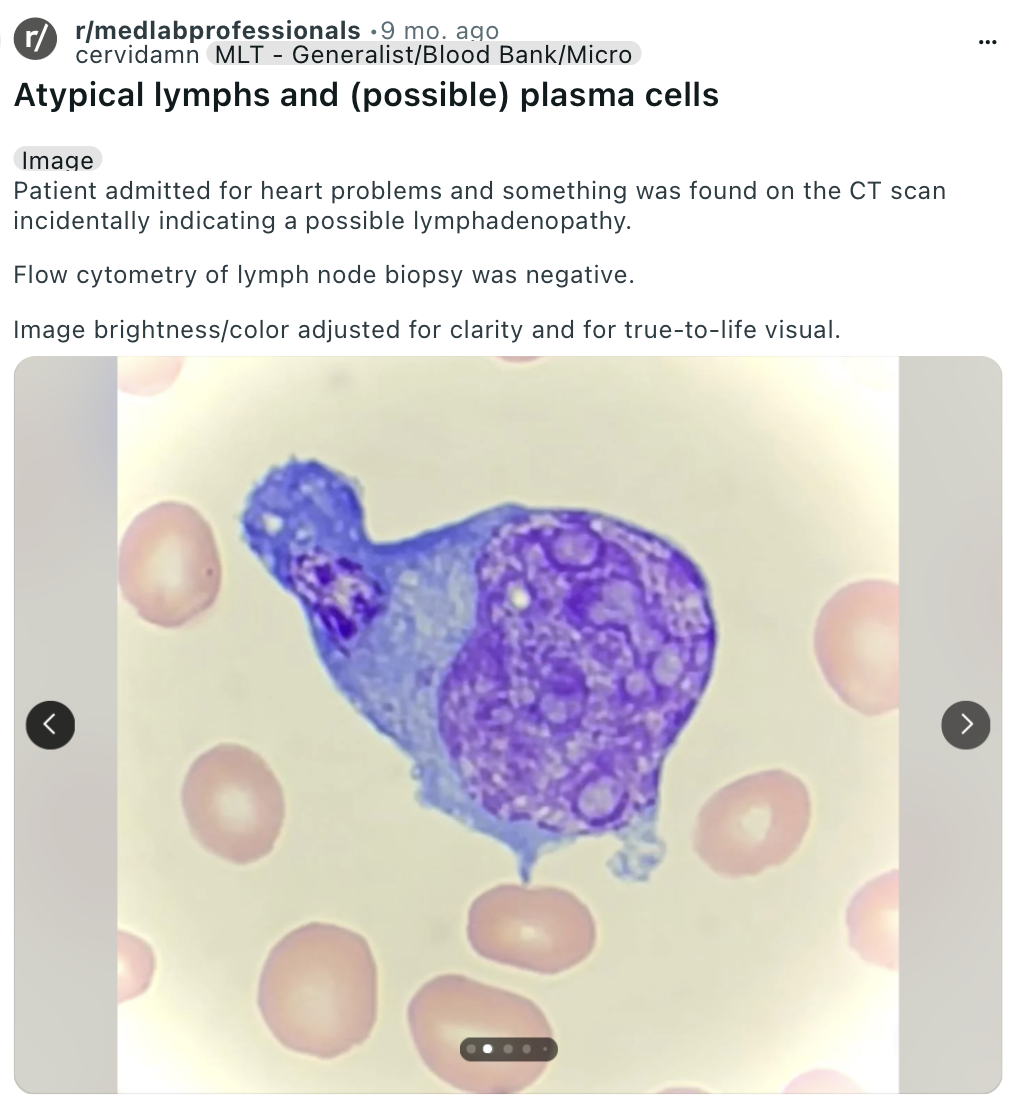
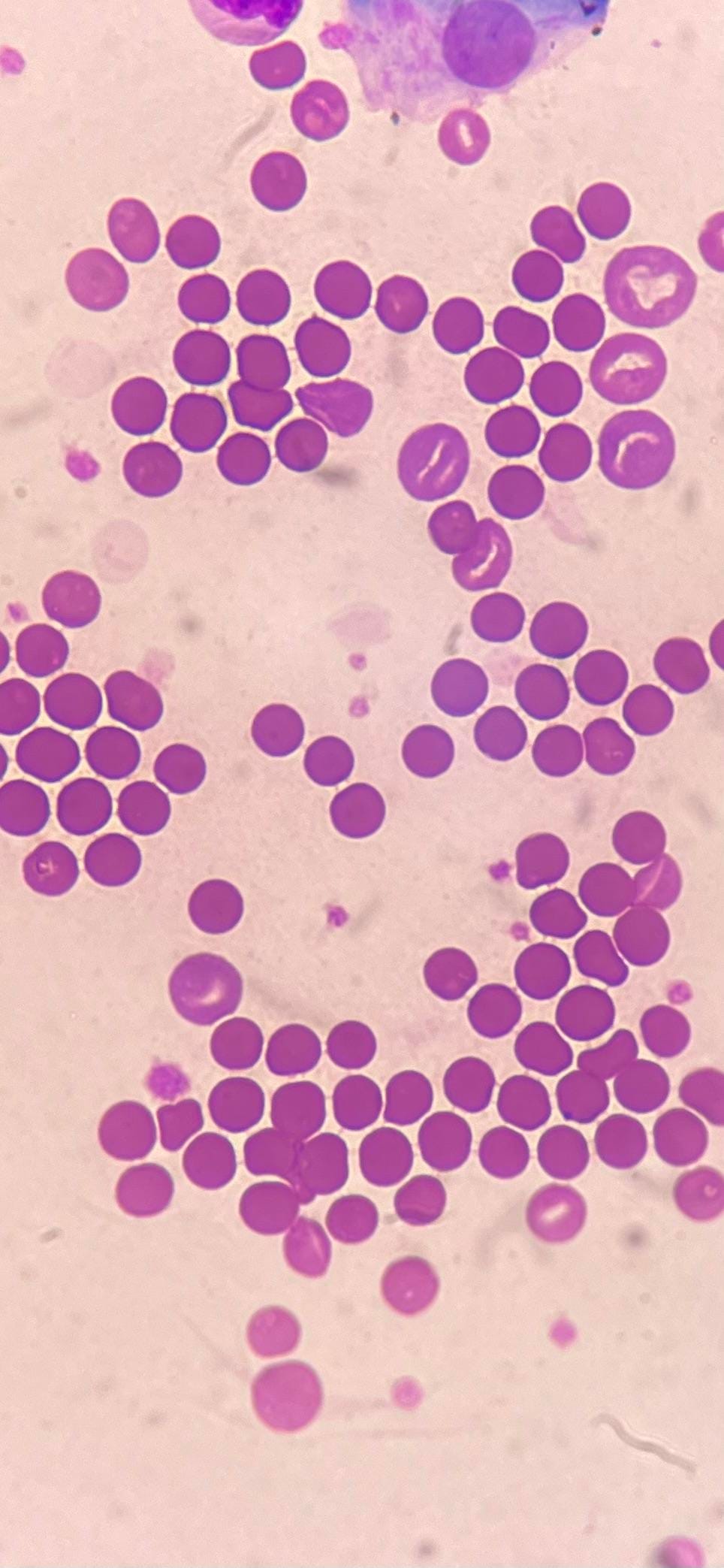
I've collected some screenshots of what I've been seeing across Reddit from the sub r/MedLabProfessionals, but we need to critically look at leukemia – what exactly it is, what is so backwards about it and how it came to be so prevalent in mankind over just a century.
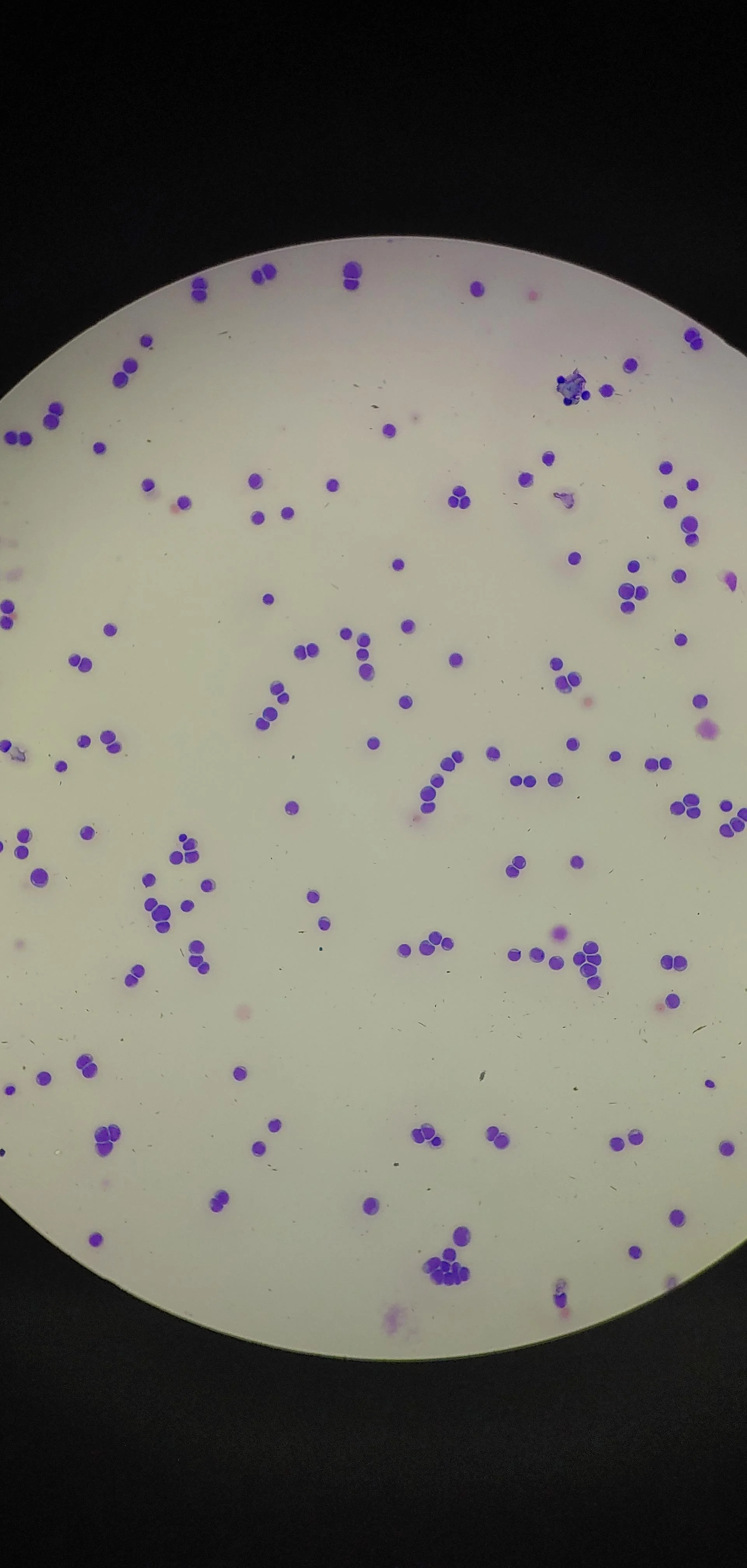
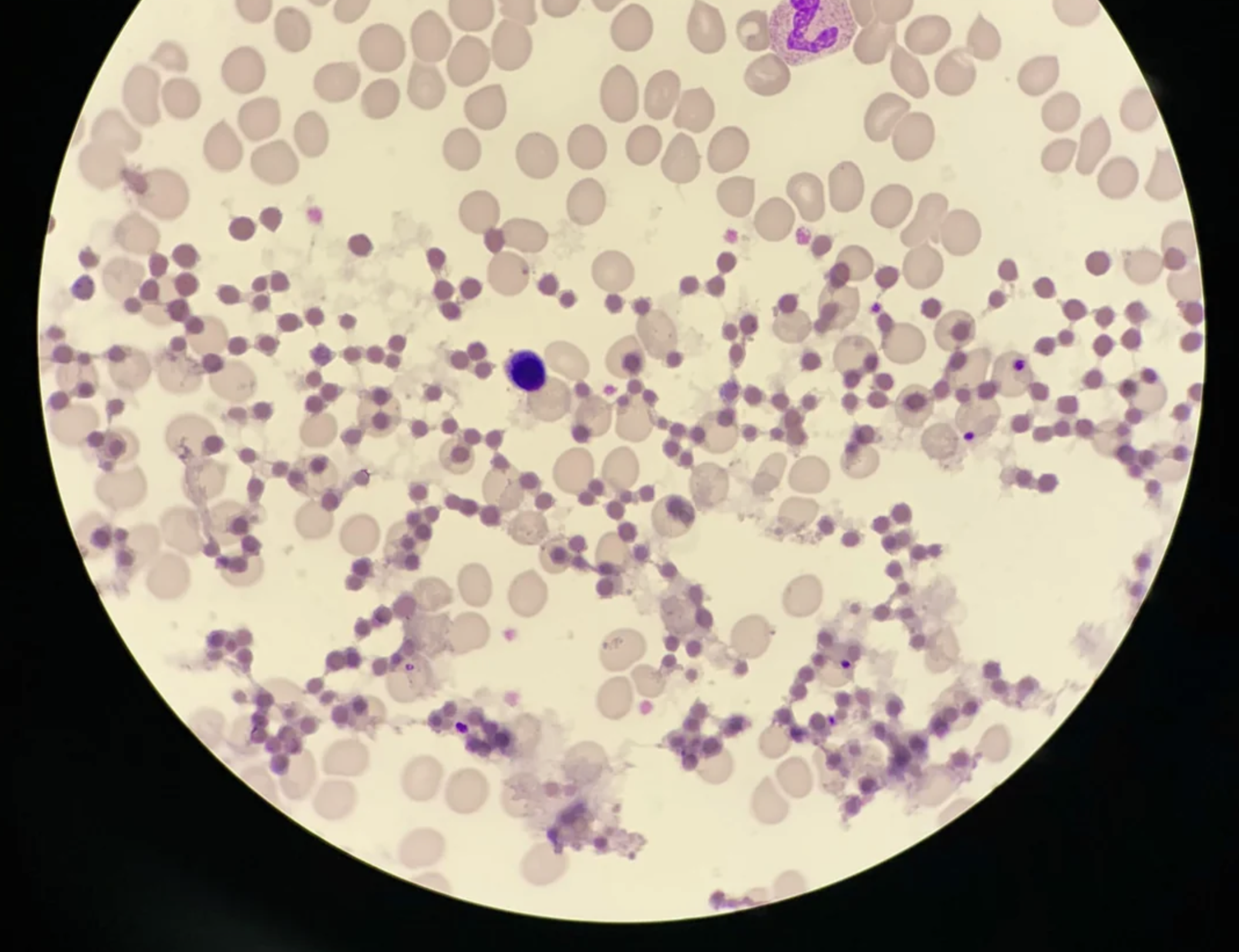
Before you go through these, know that a WBC in a healthy individual is under 11,000. Over 11,000 there is suspicion of leukemia. Over 50,000 is considered an aggressive case of leukemia. The cases you will see below are in the hundreds of thousands.
When WBC counts climb into the hundreds of thousands, we're no longer looking at a normal immune response to infection or inflammation. We're seeing a system that has lost control over cellular reproduction, differentiation, and death.

So What's Going Wrong?
The first problem is overproduction of ineffective immune cells. The bone marrow is overproducing cells that are immature or dysfunctional. What should occur only in response to an immune threat is occurring randomly and with no reason.
The next problem is clonal expansion with no regulation. This means that a single progenitor cell with a genetic or epigenetic mutation is cloning itself endlessly. These clones don’t function as true defenders, they don’t fight infection. They just accumulate.
The next problem is the loss of immune system intelligence and total breakdown of its ability to function. At 200,000+ WBC, the immune system is no longer functioning as an intelligent defense system. At 400,000+ WBC, there is an extreme and immediate risk of tumor lysis syndrome, clotting, respiratory distress, and organ failure.
The “quantity” has overwhelmed the “quality”. The immune system is no longer listening to the body. It’s producing for production’s sake, without alignment to reality or need. You have masses of cells, but they’re not coordinated, mature, or functional - they are simply creating mass destruction.
It’s like having a massive army of untrained, panicking recruits troops — no generals, no coordination, no memory.
What makes things worse is that these WBC are extremely metabolically expensive—they require a ton of resources from the body to grow and function, meaning they are stealing these resources from cells that are actually vital to our function. This is one reason leukemia patients often experience extreme fatigue, weight loss, and fevers: the body is feeding an out-of-control factory at the cost of everything else.
What's Causing Leukemia Rates To Skyrocket In Children?
Believe it or not, dozens have studies have actually found that "reduced exposure to infection in the first few months of life increases the risk of developing acute lymphoblastic leukaemia".

"The study supports the hypothesis that early common infections may play a protective role in the aetiology of childhood leukaemia."

"There were more first-born children among the patients, more children from one-child families, and more children of parents with higher education."


How Could Vaccines Lead to Leukemia?
This concern isn't theoretical—it has been discussed in hundreds of published scientific literature. DNA vaccines involve direct interaction with the host genome and long-term immune stimulation, which opens the door to insertional mutagenesis, epigenetic interference, and immune dysregulation.
"A number of controversial adverse events have, however, been purported to be associated with HBVs, including rheumatoid arthritis (RA), diabetes, demyelinating diseases (e.g., multiple sclerosis [MS]), chronic fatigue syndrome, and more recently, lymphoblastic leukaemia." [Source]
"A non-significant positive association with total shots of viral vaccinations and a weak non-significant inverse association with breast feeding were also found."

"Pre-school acute lymphoblastic leukemia (ALL) peak is consistent in developed but not in developing countries and its magnitude apparently correlates with the socioeconomic status. During the 1980s and 1990s, ALL incidence among children 1–4 years increased 1.5 times."
DNA vaccines, like the hepatitis B vaccine given hours after birth, carry double-stranded DNA into the cell nucleus—not just the cytoplasm. DNA plasmids are most likely to enter and integrate with cells that are rapidly dividing (like immune cells or bone marrow cells, especially those in growing babies). This causes the DNA to persist for long periods and allows it to integrate with large numbers of cells.
When the vaccine DNA is inserted into nuclear DNA, it's inserted within oncogenes and tumor suppressor genes. This leads to the disruption normal cell cycle control, causing unregulated clonal proliferation—a hallmark of leukemia.
I've read dozens of studies that found the hep B vaccine also inhibits apoptosis of immature lymphocytes and allows damaged or mutated clones to survive longer than they should. This means that over time pre-leukemic clones are able to expand unchecked, especially in children with early vaccination schedules.
There are even studies which found a significant increase in incidence of childhood leukemia in regions following mass hepatitis B vaccination campaigns (France, Taiwan, US). There are also case studies of ALL (acute lymphoblastic leukemia) occurring within months of Hep B vaccination in previously healthy children.
Naturally, health authorities dismiss these occurrences as chance and claim that there is no proof that the vaccine directly causes leukemia – but that begs the question, how much evidence needs to be found for them to consider the possible connection? Why do they refuse to acknowledge the clear biological pathways by which this could occur?
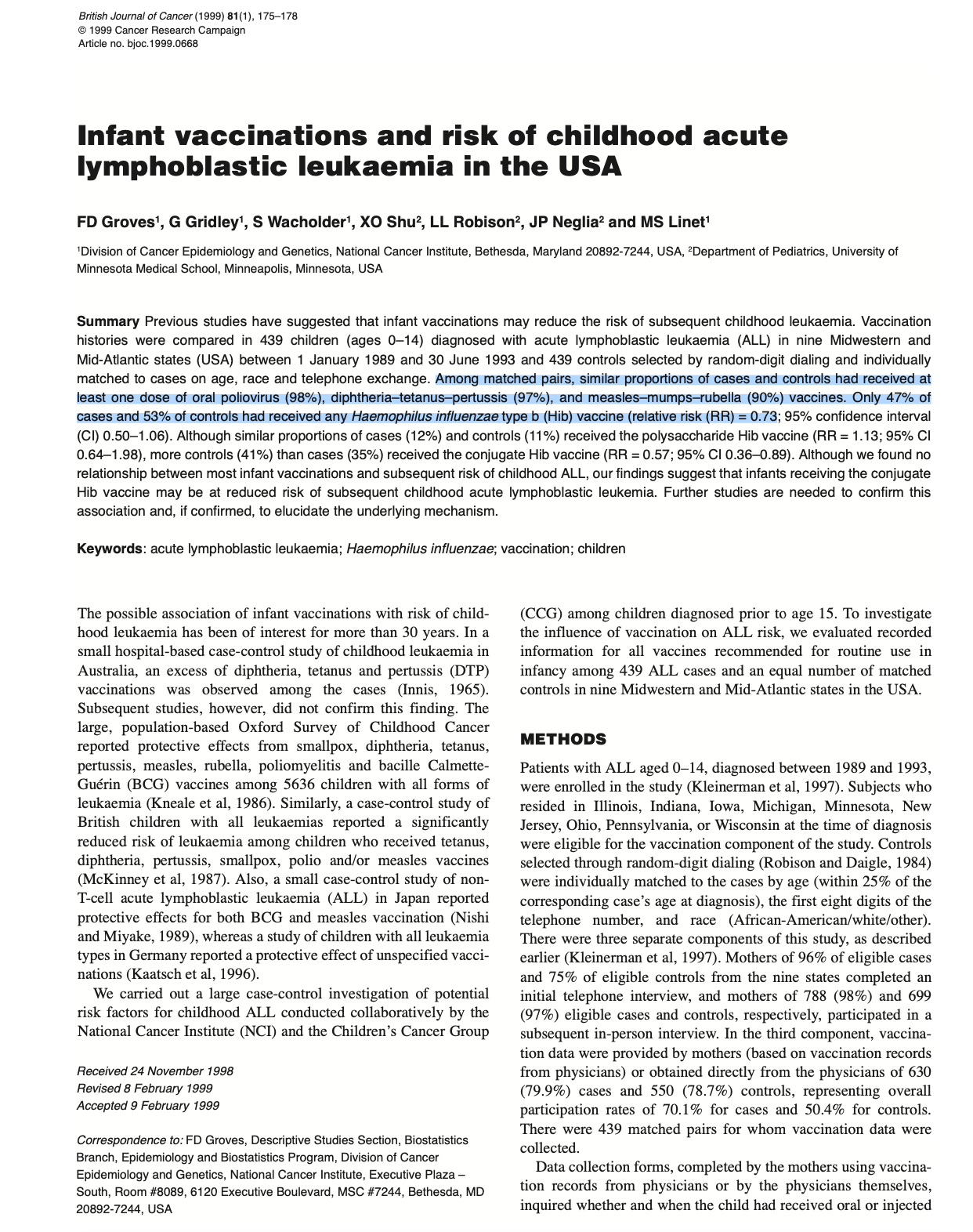
What About All Those Studies That Found Vaccines Reduced The Risk Of Leukemia In Children?
Almost every single study supporting the use of vaccines as protection from leukemia are extremely skewed and manipulative in the way that they present data.
Take the study below for example, which confidently claims that vaccination reduces incidence of leukemia.
But if you read closely, you see that the study does not compare vaccinated vs. unvaccinated children– instead it compared only between children who received two or fewer doses and children who received three or more doses.
But the group receiving "≤2 doses" is still vaccinated. So if vaccination itself did increase leukemia risk, then both groups could be at higher risk than truly unvaccinated children - and we would never know it.
By removing the unvaccinated baseline, the study erases any ability to detect absolute risk introduced by the vaccine.
Not only does the study fail to assess the true risk between the vaccinated and unvaccinated (which is, by the way, the most common way I've seen studies skew results and still claim vaccination is effective at protecting against ___), it also fails to analyze the latency period (time from vaccination to disease onset).
Here is another good example of a study that completely manipulates data to present a misleading conclusion:
This study didn't track whether each child was vaccinated. Instead, it measured county-level vaccination coverage and assumed that individuals in high-coverage counties were more likely to be vaccinated. This creates misclassification bias, you can’t infer personal-level risk (of leukemia) from group-level exposure (county vaccination rate).
The study also doesn’t compare vaccinated vs unvaccinated children at all - instead it compares children born in regions with “higher” vs. “lower” vaccination rates. Even counties with “low” vaccination rates are still highly vaccinated. This ensures nearly all children in the study are vaccinated, making it impossible to see any absolute risk of vaccination.
They also decided to remove all leukemia and cancer cases diagnosed before age 2 from the analysis (~1,063 cases). This exclusion removes the most temporally relevant and acute-onset cases—which are most likely to show an association with early-life vaccinations.
Many vaccine reactions or immune disruptions occur within the first year of life, especially following multi-dose regimens. By removing early cases, the study introduces survivorship bias: only children healthy enough to reach age 2 are included.
The study claims that vaccination reduces leukemia risk despite the data not truly supporting that claim. For example, an OR of 0.84 (95% CI 0.70–1.00) is statistically fragile - yet framed as protective. Yet other more significant findings are ignored or entirely downplayed - like the increased risk of medulloblastoma with higher Hib rates (OR = 1.62), and increased risk of NHL with higher MMR rates (OR = 2.81).
It also makes the claim of vaccines providing protection without explaining how the they do so. Without a biological mechanism, the claim rests entirely on statistical associations, which can be easily manipulated. A proper study should explore how the vaccine interacts with immune cells, bone marrow, or DNA repair mechanisms.
Let's do one more study for good measure:

Once again, this study only compares children who received specific vaccines (e.g. Hib) to children who received other vaccines or none of that specific type. Nearly all children in the study were vaccinated (e.g., 98% received polio, 97% DTP). Without a truly unvaccinated control group, the baseline risk of leukemia cannot be accurately assessed.
Many vaccine studies conclude there is no increased leukemia risk, or even suggest a protective effect. However, multiple study design choices can obscure a real biological risk. Below is a summary of the most common ways this manipulation or misrepresentation can occur:
Healthy User Bias
Families that vaccinate fully tend to have better nutrition, healthcare access, and fewer environmental risks. These unrelated advantages lower leukemia risk and make vaccines appear protective.
Reverse Causation
Pre-leukemic symptoms may delay or reduce vaccinations. When leukemia is diagnosed later, these kids appear 'under-vaccinated,' flipping the direction of cause and effect.
Confounding by Healthcare Access
Unvaccinated children may face higher environmental toxin exposure or poorer medical care. These real leukemia risk factors are mistaken as effects of not vaccinating.
Misclassification
Leukemia symptoms can be confused with infection early on. Children may be misdiagnosed and vaccinated further, obscuring early adverse effects.
Overadjustment in Models
Researchers may 'adjust away' real signals by including variables like infection history or medical visits, which are influenced by both vaccination and early disease.
Narrow Outcome Definitions
Studies may only include ALL, excluding other leukemia subtypes or immune disorders triggered by vaccination.
Time Window Manipulation
Excluding cases that develop soon after vaccination or limiting exposure windows can miss acute leukemia onset.
Publication Bias
Null or negative findings are more likely to be published, especially when tied to pharma funding or policy agendas.











Discussion